
A Case of Molluscum Contagiosum in an Adult Patient with Rheumatoid Arthritis, Following Combination Therapy with Adalimumab, Methotrexate and Prednisolone
Seok Hoon Moon, Sang Hyun Cho, Jeong Deuk Lee and Hei Sung Kim*
- Department of Dermatology, Catholic University of Korea, Incheon St. Mary’s Hospital, Incheon, Korea
*Address for Correspondence: Hei Sung Kim, Department of Dermatology, Catholic University of Korea, Incheon St. Mary’s Hospital, Incheon, Korea, Tel: 82-32-280-5700; E-mail: hazelkimhoho@gmail.com
Citation: Moon SH, Cho SH, Lee JD, Kim HS. A Case of Molluscum Contagiosum in an Adult Patient with Rheumatoid Arthritis, Following Combination Therapy with Adalimumab, Methotrexate and Prednisolone. J Clin Investigat Dermatol. 2016;4(2): 2.
Copyright © 2016 Kim S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 4, Issue: 2
Submission: 19 September, 2016| Accepted: 23 September, 2016| Published: 03 October, 2016
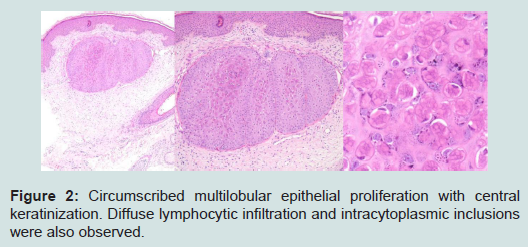
A 46-years old female was referred from the rheumatology department with diffuse skin lesions. She had been diagnosed with rheumatoid arthritis in 2006 and initially underwent treatment with a combined regimen of methotrexate (MTX, 12.5 mg per week), prednisolone (2.5 mg per day) and leflunomide (10 mg per day). Dueto the poor response, leflunomide was substituted to adalimumab (40 mg every other week) in September 2014 after negative screening for viral hepatitis and tuberculosis. 6 months into the combined therapy of adalimumab, prednisolone and methotrexate, the patient developed multiple, tiny erythematous to skin-colored papules and referred to the department of dermatology. On close examination, she presented with tender and pruritic, multiple, 0.1-0.2 cm-sized, slightly erythematous papules on the mons pubis and the Lt. lower leg (Figure 1). The patient was HIV negative and her laboratory assessment was normal. Molluscum contagiosum infection was suspected after curettage but a punch biopsy was performed from the the mons pubis and the left lower leg for confirmation. The histopathologic examination showed circumscribed multilobular epithelial proliferation with central keratinization. Diffuse lymphocytic infiltration and intracytoplasmic inclusions were also observed (Figure 2). Based on clinical and pathologic findings, diagnosis of diffuse molluscum contagiosum was made. To prevent further spread of the molluscum, adalimumab was withdrawn from the regimen. Although we explained the possibility of persistence and spread of the molluscum lesions, the patient refused to undergo extraction of the lesions. No recurrence of molluscum from the biopsy site or further spreading was observed at 8 months follow-up.

1]. TNF-α plays a critical role in immune response to viral infection. When inhibited, the function of phagocytes, dendritic cells and T lymphocytes may be impaired. Furthermore, TNF-α is important in signaling apoptosis in infected cells [2]. Molluscum contagiosum has been shown to interfere with the TNF-receptor 1 apoptotic signaling pathways and thereby inhibits apoptosis of the virus-infected cells [3]. There are few reports of multiple molluscum contagiosum infection in relation to TNF inhibitors [2,4] but theoretically, the host’s natural antiviral mechanisms may be compromised in patients receiving TNF inhibitors. This may explain the occurrence of multiple molluscum contagiosum in an otherwise immunocompetent patient.
Although this is a single case report, the time sequence of initiation of adalimumab and the occurrence of molluscum contagiosum, the pathophysiologic plausibility, and the absence of further spread after cessation of adalimumab favor the relationship between adalimumaband molluscum contagiosum infection. Since molluscum contagiosum is a benign lesion, it tends to be overlooked by physicians. Physicians should be aware of the possibility of molluscum contagiosum infection in patients receiving TNF inhibitors and consider switching TNF inhibitors to other medication in such cases.
Acknowledgements
The authors acknowledge the support provided by Brazilian Funding Agencies: BNDES (09.2.1458.1); FINEP; Capes; and grant 2013/07276-1 (CEPOF). We are also grateful to MM Optics and PDT Pharma.References
- Vora RV, Pilani AP, Kota RK (2015) Extensive giant molluscum contagiosum in a HIV positive patient. J Clin Diagn Res 9: WD01-WD02.
- Antoniou C, Kosmadaki MG, Stratigos AJ, Katsambas AD (2008) Genital HPV lesions and molluscum contagiosum occurring in patients receiving anti-TNF-alpha therapy. Dermatology 216: 364-365.
- Hu S, Vincenz C, Buller M, Dixit VM (1997) A novel family of viral death effector domain-containing molecules that inhibit both CD-95- and tumor necrosis factor receptor-1-induced apoptosis. J Biol Chem 272: 9621-9624.
- Cursiefen C, Grunke M, Dechant C, Antoni C, Jünemann A, et al. (2002) Multiple bilateral eyelid molluscum contagiosum lesions associated with TNFalpha-antibody and methotrexate therapy. Am J Ophthalmol 134: 270-271.