
Case Report
*Address for Correspondence: Karolyn Wanat, Department of Dermatology, University of Iowa, 200 Hawkins Drive, Iowa City, Iowa, 52242, USA, Tel: 319-356-1694; Fax: 319-356-0349 E-mail: Karolyn-Wanat@uiowa.edu
Citation: Shields B, Tschetter A, Liu V, Wanat KA. Erosive Papulonodular Dermatosis of the Lower Extremities: A Reactive Change in the Setting of Chronic Lymphedema. J Clin Investigat Dermatol. 2016;4(1): 3.
Copyright © 2016 Shields B, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 4, Issue: 1
Submission: 23 May, 2016| Accepted: 04 June, 2016 | Published: 08 June, 2016

 EPD is considered an inflammatory cutaneous eruption secondary to a chronic, external irritant and includes the previously distinct entities of perianal pseudoverrucous papules and nodules, granuloma gluteale infantum, and Jacquet erosive dermatitis [1,2]. Papulonodules are classically found in the diaper area and at urostomy and colostomy sites following repeated leakage, encopresis or urinary incontinence [1]. However, striking cases have been reported in less common locations secondary to post-operative inflammation combined with an occlusive wound dressing [2], and following continuous wear of medical examination gloves due to an underlying delusion [4]. While presenting in atypical sites, both cases highlight occlusion as is common in EPD. In our case, the typical papules of EPD arose secondary to protein-rich lymphatic fluid in the setting of chronic lymphedema in the absence of occlusion. Elephantiasis nostra verrucosa is a more frequent complication of longstanding lymphedema and also demonstrates pseudoepitheliomatous hyperplasia on biopsy [5,6]. Our case is differentiated from ENV clinically by the presence of moist, red papules and nodules with erosions, and histopathologically by the absence of dermal and subcutaneous woody fibrosis, as well as by the maintenance of the dermal papillae, eccrine glands and elastic fibers [5,6].
EPD is considered an inflammatory cutaneous eruption secondary to a chronic, external irritant and includes the previously distinct entities of perianal pseudoverrucous papules and nodules, granuloma gluteale infantum, and Jacquet erosive dermatitis [1,2]. Papulonodules are classically found in the diaper area and at urostomy and colostomy sites following repeated leakage, encopresis or urinary incontinence [1]. However, striking cases have been reported in less common locations secondary to post-operative inflammation combined with an occlusive wound dressing [2], and following continuous wear of medical examination gloves due to an underlying delusion [4]. While presenting in atypical sites, both cases highlight occlusion as is common in EPD. In our case, the typical papules of EPD arose secondary to protein-rich lymphatic fluid in the setting of chronic lymphedema in the absence of occlusion. Elephantiasis nostra verrucosa is a more frequent complication of longstanding lymphedema and also demonstrates pseudoepitheliomatous hyperplasia on biopsy [5,6]. Our case is differentiated from ENV clinically by the presence of moist, red papules and nodules with erosions, and histopathologically by the absence of dermal and subcutaneous woody fibrosis, as well as by the maintenance of the dermal papillae, eccrine glands and elastic fibers [5,6].
Erosive Papulonodular Dermatosis of the Lower Extremities: A Reactive Change in the Setting of Chronic Lymphedema
Bridget Shields1, Amanda Tschetter2, Vincent Liu2 and Karolyn A. Wanat2*
- 1Department of Internal Medicine, Iowa Methodist Medical Center, Des Moines, IA, USA
- 2Department of Dermatology, University of Iowa, 200 Hawkins Drive, Iowa City, Iowa, 52242, USA
*Address for Correspondence: Karolyn Wanat, Department of Dermatology, University of Iowa, 200 Hawkins Drive, Iowa City, Iowa, 52242, USA, Tel: 319-356-1694; Fax: 319-356-0349 E-mail: Karolyn-Wanat@uiowa.edu
Citation: Shields B, Tschetter A, Liu V, Wanat KA. Erosive Papulonodular Dermatosis of the Lower Extremities: A Reactive Change in the Setting of Chronic Lymphedema. J Clin Investigat Dermatol. 2016;4(1): 3.
Copyright © 2016 Shields B, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 4, Issue: 1
Submission: 23 May, 2016| Accepted: 04 June, 2016 | Published: 08 June, 2016
Keywords
Dermatitis; Wound healing; LymphedemaAbstract
Erosive papulodnodular dermatosis (EPD) is classified as an inflammatory cutaneous eruption secondary to a chronic, external irritant [1,2]. Treatment for EPD focuses on eliminating the presumed irritant [2] and preventing secondary bacterial infection [1,3]. We present a case of EPD, secondary to inflammation from lymphatic stasis, refractory to medical and antimicrobial treatment. Given the recalcitrant nature, sharp surgical debridement followed by Unnaboot application, significant diuresis and weight loss resulted in remarkable improvement. We report an instructive case of erosive papulonodular dermatosis secondary to inflammation associated with lymphatic stasis to alert clinicians of this rare presentation and causative agent. Further, this case warrants discussion regarding surgical therapy as a potential adjunctive therapy to accelerate healing in EPD.Abbreviations
EPD: Erosive Papulonodular Dermatosis; ENV: Elephantiasis Nostra VerrucosaReport of a Case
A woman in her fifties with diastolic congestive heart failure, diabetes mellitus type II, obstructive sleep apnea (on continuous positive airway pressure), and hypertension presented to our clinic for evaluation of lower extremity wounds refractory to treatment. Six months prior to presentation she noted increasing edema with severe pruritus and pain along the right anterior tibia resulting in the development of painful papules. Doppler ultrasound did not reveal venous insufficiency. Prior unsuccessful treatments included acetic acid soaks, sequential compression devices, compression stockings, massage, and elevation. Wound cultures were remarkable for polymicrobial growth, including Candida parapsilosis, methicillin resistant Staphylococcus aureus, Enterococcus, Streptococcus, Aerococcus, and Pseudomonas species. However, treatment with numerous antimicrobials did not result in improvement. She received hydrocodone-acetaminophen, pregabalin, and duloxetine for associated pain.Physical examination revealed weeping, flat-topped, pink papules coalescing into cobblestoned plaques on the right shin (Figure 1A) and smaller papules on the left shin with surroundingsignificant woody edema. Repeat wound cultures were positive for Pseudomonas aeruginosa and Candida parapsilosis. Evaluation of a punch biopsy revealed parakeratotic, spongiotic epidermal, verruci form hyperplasia with prominent dermal edema, fibroplasia, and a superficial, mixed, perivascular infiltrate (Figure 2) maintenance of the dermal papillae, eccrine glands and elastic fibers. The histopathologic picture supported the clinical diagnosis of erosive papulonodular dermatosis (EPD); however, arising in the setting of chronic lymphedema, elephantiasis nostra verrucosa (ENV) was also considered.
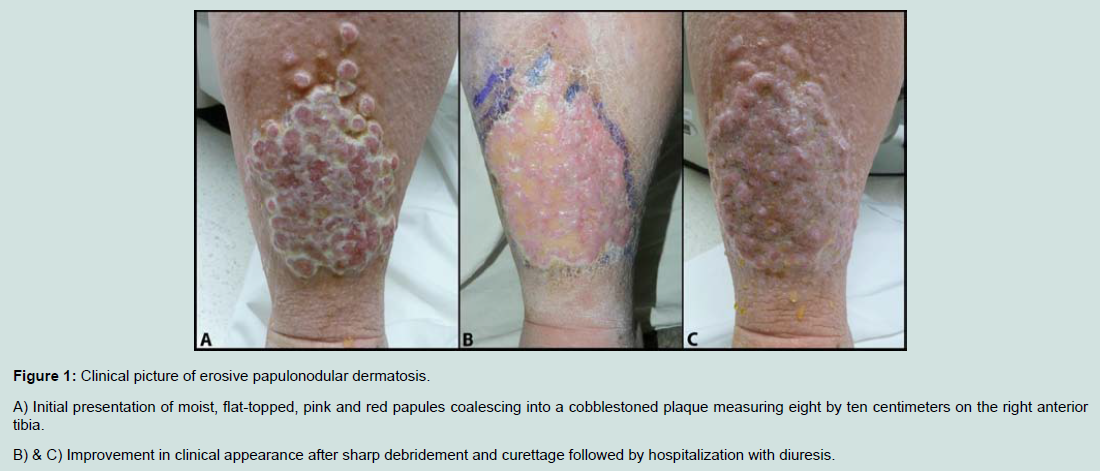
Figure 1A: Clinical picture of erosive papulonodular dermatosis.A) Initial presentation of moist, flat-topped, pink and red papules coalescing into a cobblestoned plaque measuring eight by ten centimeters on the right anterior tibia.B) & C) Improvement in clinical appearance after sharp debridement and curettage followed by hospitalization with diuresis.
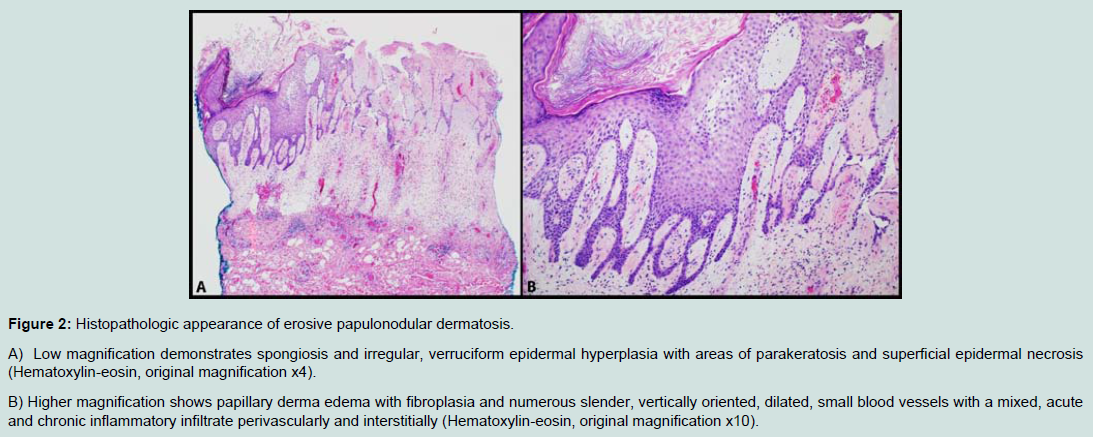
Figure 2: Histopathologic appearance of erosive papulonodular dermatosis.A) Low magnification demonstrates spongiosis and irregular, verruciform epidermal hyperplasia with areas of parakeratosis and superficial epidermal necrosis (Hematoxylin-eosin, original magnification x4).B) Higher magnification shows papillary derma edema with fibroplasia and numerous slender, vertically oriented, dilated, small blood vessels with a mixed, acute and chronic inflammatory infiltrate perivascularly and interstitially (Hematoxylin-eosin, original magnification x10).
Treatment for EPD centers on eliminating the irritant (commonly urine, feces, or chronic moisture) [2], preventing secondary bacterial infection, and removing precipitating factors in an attempt to recover skin barrier function [1,3]. Unfortunately, in this case the combination of uncontrolled congestive heart failure resulting in edema, peripheral neuropathy, and chronic pain, made removal of the irritating lymphatic drainage difficult. Medical attempts at thinning the papules and nodules with elevation, aggressive compression, silver nitrate, and high potency corticosteroids, in addition to eliminating superinfection with gentian violet and dilute acetic acid soaks, were unsuccessful. Given the refractory nature, sharp surgical debridement followed by Unna boot application (gentian violet, Adaptic®, calcium alginate dressing, Unna wrap) was attempted. Subsequent hospitalization for congestive heart failureresulted in diuresis and a fifty-pound weight loss with remarkable improvement (Figure 1B). The contralateral leg had significantly smaller papules and nodules that were not surgically debrided and exhibited modest improvement with diuresis. Unfortunately, poor control of her underlying comorbidities has resulted in continuedlymphatic drainage preventing complete resolution.
We report an instructive case of erosive papulonodular dermatosis secondary to inflammation from chronic lymphatic stasis to alert clinicians of this unique presentation. Furthermore, our patient underscores how surgical intervention may be a beneficial adjunctivetherapy to aid in healing in EPD. However, caution is warranted with excisional techniques as limited documentation exists reporting favorable long-term results when used in patients with extensive lymphedema. Staged excisional therapy, if performed improperly, may actually do more harm than good. Conservative treatment remains first line treatment for chronic lymphedema and its sequelae.
References
- Robson KJ, Maughan JA, Purcell SD, Petersen MJ, Haefner HK, et al. (2006) Erosive papulonodular dermatosis associated with topical benzocaine: a report of two cases and evidence that granuloma gluteale, pseudoverrucous papules, and Jacquet's erosive dermatitis are a disease spectrum. J Am Acad Dermatol 55(5 Suppl): S74-S80.
- Ferguson NN, Wendel A, Farah R, Liu V, Swick BL (2013) Postsurgical erosive papulonodular dermatosis. J Am Acad Dermatol 69: e188-189.
- Dandale A, Dhurat R, Ghate S (2013) Perianal pseudoverrucous papules and nodules. Indian J Sex Transm Dis 34: 44-46.
- Nelson J, Maroon M (2011) Images in clinical medicine. Pseudoverrucous papules. N Engl J Med 364: e50.
- Sisto K, Khachemoune A (2008) Elephantiasis nostras verrucosa: a review. Am J Clin Dermatol 9: 141-146.
- Schissel DJ, Hivnor C, Elston DM (1998) Elephantiasis nostras verrucosa. Cutis 62: 77-80.