
Case Report
*Address for Correspondence: Samer Ghosn, MD, Department of Dermatology, American University of Beirut Medical Center, Riad El Solh St, Beirut, Lebanon, P.O.Box 11-0236, Tel: +961-1-350000, ext. 5333; Fax: +961-1-745320; E-mail: sg03@aub.edu.lb
Citation: Abbas O, Kanj N, Kurban M, Kibbi AG, Ghosn S. Atypical Necrobiotic Xanthogranuloma Associated with Epidermodysplasia Verruciformis. J Clin Investigat Dermatol. 2014;2(3): 3.
Copyright © 2014 Ghosn et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 2, Issue: 3
Submission: 01 October 2014| Accepted: 27 November 2014 | Published: 02 December 2014
Reviewed & Approved by: Dr. Kyoung-Chan Park, Professor, Department of Dermatology, Seoul National University Bundang Hospital, Korea

Atypical Necrobiotic Xanthogranuloma Associated with Epidermodysplasia Verruciformis
Ossama Abbas, Nadim Kanj, Mazen Kurban, Abdul Ghani Kibbi and Samer Ghosn*
- Department of Dermatology, American University of Beirut Medical Center, Beirut, Lebanon
*Address for Correspondence: Samer Ghosn, MD, Department of Dermatology, American University of Beirut Medical Center, Riad El Solh St, Beirut, Lebanon, P.O.Box 11-0236, Tel: +961-1-350000, ext. 5333; Fax: +961-1-745320; E-mail: sg03@aub.edu.lb
Citation: Abbas O, Kanj N, Kurban M, Kibbi AG, Ghosn S. Atypical Necrobiotic Xanthogranuloma Associated with Epidermodysplasia Verruciformis. J Clin Investigat Dermatol. 2014;2(3): 3.
Copyright © 2014 Ghosn et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Investigative Dermatology | ISSN: 2373-1044 | Volume: 2, Issue: 3
Submission: 01 October 2014| Accepted: 27 November 2014 | Published: 02 December 2014
Reviewed & Approved by: Dr. Kyoung-Chan Park, Professor, Department of Dermatology, Seoul National University Bundang Hospital, Korea
Abstract
Necrobiotic xanthogranuloma is a rare, idiopathic, and chronic systemic granulomatous disorder that is usually associated with paraproteinemia of the immunoglobulin (Ig)G kappa (κ) type. It is clinically characterized by yellowish red-to-brown indurated often ulcerating nodules or plaques that usually involve the periorbital regions of the elderly. We report an atypical case of NXG affecting only the left leg of an adolescent girl with both IgG kappa and Lambda paraproteinemias. In addition, she had associated epidemodysplasia verruciformis and severe lung disease.Keywords
Necrobiotic xanthogranuloma; Epidermodysplasia erruciformis; Paraproteinemia; Lung diseaseIntroduction
First described by Kossard and Winkelmann in 1980 [1], ecrobiotic xanthogranuloma (NXG) is a rare, chronic, idiopathic, progressive, locally destructive, systemic histiocytic disorder affecting primarily the skin. It is clinically characterized by yellowish red-tobrown indurated nodules or plaques which often ulcerate, usually involving the face and in particular upper and lower lids of elderly people. The trunk and the extremities are far less frequently involved. Majority of patients have an elevated erythrocyte sedimentation rate, leucopenia, and an IgG kappa gammopathy (in more than 80% of cases) [2]. Involvement of internal organs such as the heart, lungs, intestines, and eyes has also been reported [3,4]. We report an atypical case of NXG affecting only the left leg of an adolescent girl with both IgG kappa and Lambda paraproteinemias. In addition, the patient had associated epidemodysplasia verruciformis (EDV) and severe lung disease.Case Report
A 17-year-old girl, with history of recurrent respiratory infections and obstructive pulmonary disease, was admitted to our institution for the management of cough and respiratory failure. We were consulted to evaluate an asymptomatic, persistent, occasionally oozing lesion on the left leg of 1-year duration. In addition, she had persistent extensive asymptomatic lesions on the extremities since early childhood. Family history was positive for epidemodysplasia verruciformis (EDV) in her brother (documented by skin biopsy) and negative for atopy, immunosuppression or pulmonary diseases. She was maintained on prednisolone 5 mg per day, inhaled corticosteroids, bronchodilators, and leukotriene inhibitors for her pulmonary disease. Skin examination revealed multiple variably-sized, yellowish/dusky, atrophic, focally ulcerated and deeply infiltrated plaques with telangiectatic surface on the left leg (Figure 1A). In addition, she had numerous flat topped and verrucous skin-colored to erythematous slightly scaly papules and plaques on the trunk and extremities (Figure 1B).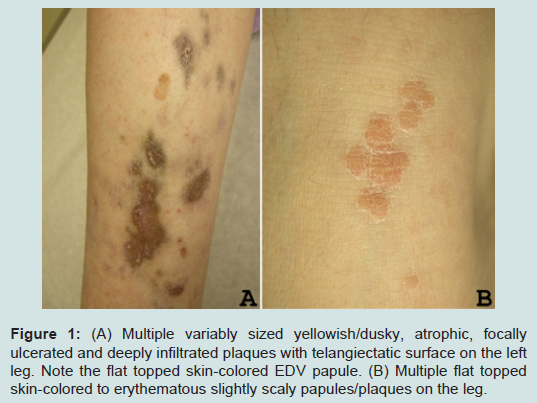
Figure 1: (A) Multiple variably sized yellowish/dusky, atrophic, focally ulcerated and deeply infiltrated plaques with telangiectatic surface on the left leg. Note the flat topped skin-colored EDV papule. (B) Multiple flat topped skin-colored to erythematous slightly scaly papules/plaques on the leg.
Histology of the left leg dusky plaque exhibited mid-dermal large acellular necrobiotic areas containing numerous cholesterol clefts and calcium deposits and surrounded by dense lymphohistiocytic infiltrate with scattered foamy macrophages (Figures 2A-2C). Special stains (including Gram, Fite, and Periodic Acid Schiff) for common bacterial/mycobacterial and fungal infections, and culture studies were all negative. The rest of her studies including fasting blood sugar and oral glucose tolerance test were all within normal. Based on these findings, a diagnosis of NXG was suspected and confirmed by the detection of both IgG kappa and Lambda paraproteinemias by serum protein immunofixation. Chest CT scan showed diffuse pan-acinar emphysematous changes and cystic bronchiectasis of the lower lobes. Full infectious work-up including lung aspirate and blood cultures was negative. A lung biopsy could not be performed due to the deteriorating respiratory condition of the patient.
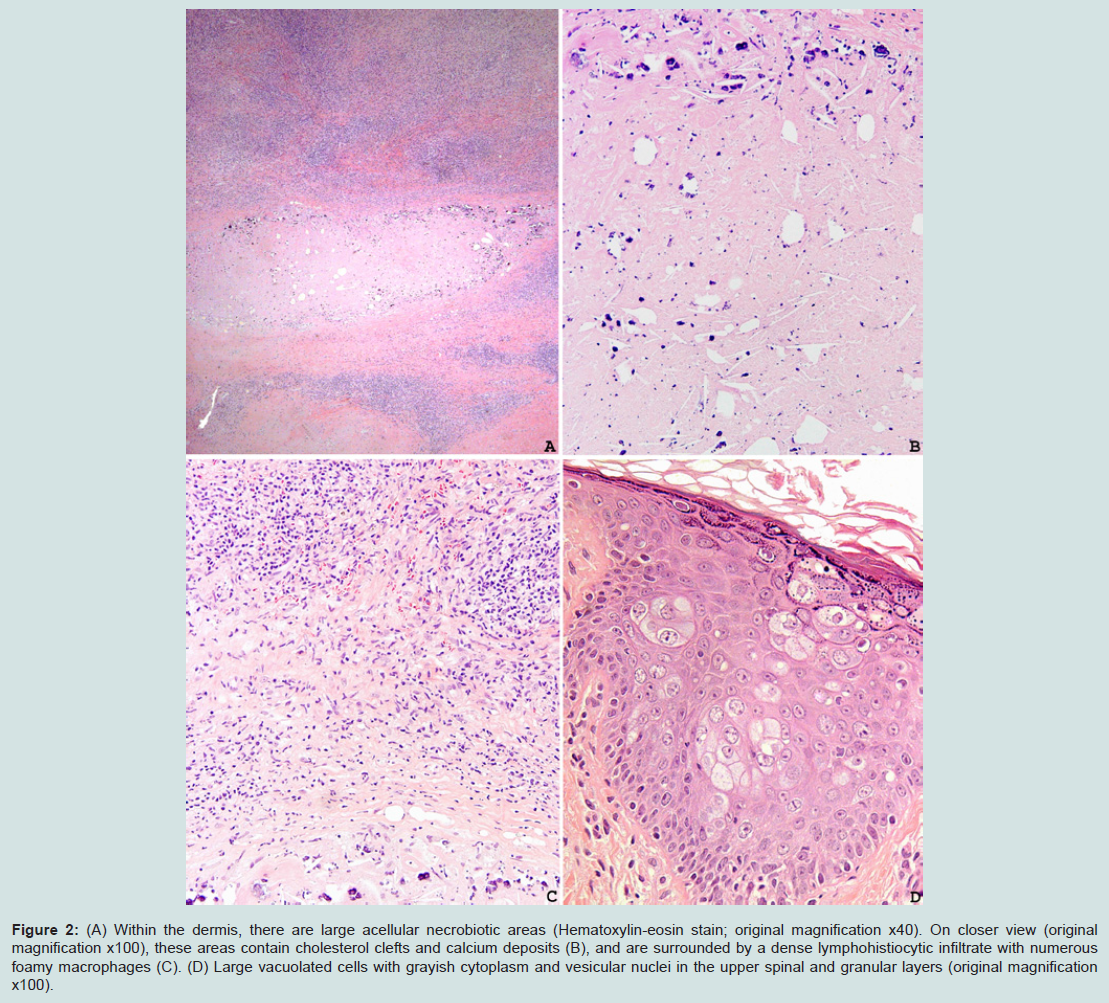
Figure 2: (A) Within the dermis, there are large acellular necrobiotic areas (Hematoxylin-eosin stain; original magnification x40). On closer view (original magnification x100), these areas contain cholesterol clefts and calcium deposits (B), and are surrounded by a dense lymphohistiocytic infiltrate with numerous foamy macrophages (C). (D) Large vacuolated cells with grayish cytoplasm and vesicular nuclei in the upper spinal and granular layers (original magnification x100).
Histology of an erythematous flat papule on the arm revealed orthokeratosis, mild papillomatosis, hypergranulosis, and large vacuolated cells with grayish cytoplasm and vesicular nuclei in the upper spinal and granular layers; changes characteristic of EDV (Figure 2D).
Discussion
NXG affects the periorbital area in more than 80% of the cases and infrequently simultaneous involvement of the trunk and extremities may occur [4,5]. Rarely, the extremities can be affected without periorbital involvement [4-7]. More than 80% of NXG cases are associated with paraproteinemia usually of the IgG kappa type, although NXG may rarely be associated with two monoclonal paraproteins [4-6]. In addition, NXG may affect visceral organs such as the lungs with severe asthma being the most well-documented association; however, most of these cases had orbital NXG [5]. Rarely, NXG has been associated with other conditions such as small lymphocytic lymphoma and Sjögren syndrome in one patient [8], Waldenström macroglobulinemia [9], and frank multiple myeloma [10]. The pathophysiology of NXG remains unknown. Many have considered NXG to be a rare reactive inflammatory complication of a persistently high paraprotein [11]. Lately, Zelger et al. have suggested an infectious etiology after they detected Borrelia burgdorferi in 6 of 7 patients with NXG [12]. In general, the disease has a progressive course and the prognosis depends on the extent of extracutaneous involvement [5]. Although well-established therapeutic modalities are lacking, chemotherapy may be effective in inducing remission of the paraproteinemia and skin lesions [12]. While combinations of alkylating agents and systemic steroids are the most commonly reported modality, systemic steroids alone are minimally effective and associated with quick relapses [2]. Other treatments include psoralen with ultaviolet A (PUVA) [13], intravenous immunoglobulin [14], thalidomide [15], clorambucil [16], and lenalidomide [17]. Surgical excision is an option in certain cases [18].In the differential diagnosis of this case, necrobiosis lipoidica was considered because of the location of the lesions and the findings on histology of extensive pandermal necrobiotic palisading granulomatous dermatitis, but was ruled out based on the histological presence of numerous cholesterol clefts, the association with paraproteinemia and the absence of diabetic diathesis. Multinucleated giant cells, often seen on histology in NXG, were not observed in the current case. In a recent study by Wood et al., multinucleated giant cells were not seen in 17% of NXG cases [4]. In addition, the fact that the patient was maintained on corticosteroids at the time of the biopsy might have altered the histopathological findings including the presence of giant cells. Erdheim Chester disease, a systemic eventually fatal non-Langerhans’ cell histiocytosis, was also considered. Our patient had osteoporosis due to prolonged oral steroid use but lacked the lytic osteosclerotic bony lesions on radiography characteristic of Erdheim-Chester disease. In addition, the presence of cholesterol clefts on biopsy does not support this possibility.
Our patient has many interesting features. The patient’s young age at the onset of her NXG, which usually affects the elderly population, is peculiar and has only been rarely reported [4,5]. The predilection to the leg without periorbital involvement and the association with two monoclonal paraproteins are also unusual features [19-21]. In addition, our case illustrates for the first time the concomitant occurrence of NXG and EDV, a hereditary disease manifesting as widespread warts and pityriasis versicolor-like lesions associated with various human papilloma virus (HPV) types especially HPV 5 and 8. There is evidence that EDV is associated with an abnormal immune system as patients may show no response to contact immunotherapy, and EDV-like lesions have been described in patients with defective cell-mediated immunity, including patients with organ transplantation and HIV infection [22]. This association between two relatively rare conditions is unlikely to be solely due to chance. Whether one condition predisposed to the other is hard to predict. The possibility of paraproteinemia being secondary to the immune dysregulation accompanying EDV seems plausible although abnormalities in humoral immunity have never been reported in EDV patients. Alternatively, the possibility of EDV-like lesions secondary to paraproteinemia could be rejected based on the early onset and the documented positive family history of EDV. Last, although a lung biopsy could not be done to confirm it, the patient may have had severe pulmonary disease secondary to NXG.
References
- Kossard S, Winkelmann RK (1980) Necrobiotic xanthogranuloma with paraproteinemia. J Am Acad Dermatol 3: 257-270.
- Spicknall KE, Mehregan DA (2009) Necrobiotic xanthogranuloma. Int J Dermatol 48: 1-10.
- Peyman A, Walsh N, Green P, Dorey MW, Seamone C, et al. (2012) Necrobiotic xanthogranuloma associated with necrotizing scleritis. Am J Dermatopathol 34: 644-647.
- Wood AJ, Wagner MV, Abbott JJ, Gibson LE (2009) Necrobiotic xanthogranuloma: a review of 17 cases with emphasis on clinical and pathologic correlation. Arch Dermatol 145: 279-284.
- Fernandez-Herrera J, Pedraz J (2007) Necrobiotic xanthogranuloma. Semin Cutan Med Surg 26: 108-113.
- Chave TA, Hutchinson PE (2001) Necrobiotic xanthogranuloma with two monoclonal paraproteins and no periorbital involvement at presentation. Clin Exp Dermatol 26: 493-496.
- Ghiasi N, Alavi A, Coutts PM, Ghazarian D, Sibbald RG (2012) Necrobiotic xanthogranuloma as an unusual cause of refractive chronic bilateral leg ulceration. Int J Low Extrem Wounds 11: 293-295.
- Naghashpour M, Setoodeh R, Moscinski L, Bergier G, McCardle T, et al. (2011) Nonnecrobiotic necrobiotic xanthogranuloma as an initial manifestation of paraproteinemia and small lymphocytic lymphoma in a patient with Sjogren syndrome. Am J Dermatopathol 33: 855-857.
- Balagula Y, Straus DJ, Pulitzer MP, Lacouture ME (2011) Necrobiotic xanthogranuloma associated with immunoglobulin m paraproteinemia in a patient with Waldenstrom macroglobulinemia. J Clin Oncol 29: e305-e307.
- Inthasotti S, Wanitphakdeedecha R, Manonukul J (2011) A 7-Year history of Necrobiotic xanthogranuloma following asymptomatic multiple myeloma: a case report. Dermatol Res Pract 2011: 927852.
- Whyte A, Davies A, Jenkins C (2010) Necrobiotic xanthogranuloma, a rare complication of a persistently high paraprotein. Br J Haematol 150: 1.
- Zelger B, Eisendle K, Mensing C, Zelger B (2007) Detection of spirochetal micro-organisms by focus-floating microscopy in necrobiotic xanthogranuloma. J Am Acad Dermatol 57: 1026-1030.
- Al-Niaimi FA, Dawn G, Cox NH (2010) Necrobiotic xanthogranuloma without paraproteinaemia: marked improvement with psoralen ultraviolet A treatment. Clin Exp Dermatol 35: 275-277.
- Hallermann C, Tittelbach J, Norgauer J, Ziemer M (2010) Successful treatment of necrobiotic xanthogranuloma with intravenous immunoglobulin. Arch Dermatol 146: 957-960.
- Efebera Y, Blanchard E, Allam C, Han A, Lee S, et al. (2011) Complete response to thalidomide and dexamethasone in a patient with necrobiotic xanthogranuloma associated with monoclonal gammopathy: a case report and review of the literature. Clin Lymphoma Myeloma Leuk 11: 298-302
- Ryan E, Warren LJ, Szabo F (2012) Necrobiotic xanthogranuloma: response to chlorambucil. Australas J Dermatol 53: e23-e25.
- Silapunt S, Chon SY (2010) Generalized necrobiotic xanthogranuloma successfully treated with lenalidomide. J Drugs Dermatol 9: 273-276.
- Gacto P, Barrera F, Pereyra JJ, Fernandez-Ortega P (2009) Necrobiotic xanthogranuloma: efficacy of surgery in 2 patients. Actas Dermosifiliogr 100: 499-502.
- Chave TA, Chowdhury MM, Holt PJ (2001) Recalcitrant necrobiotic xanthogranuloma responding to pulsed high-dose oral dexamethasone plus maintenance therapy with oral prednisolone. Br J Dermatol 144: 158-161.
- Hashemi P, Rashidi A, Chapas AM, Balfour EM (2012) Necrobiotic xanthogranuloma of the extremities with paraproteinemia and without periorbital involvement at presentation. Cutis 89: 41-44.
- Kawakami Y, Yamamoto T (2011) Letter: Necrobiotic xanthogranuloma of extremities in an elderly patient successfully treated with low-dose prednisolone. Dermatol Online J 17: 13.
- Daly ML, Hay RJ (2012) Epidermodysplasia verruciformis and human immunodeficiency virus infection: a distinct entity? Curr Opin Infect Dis 25: 123-125.