
Journal of Cardiobiology
Download PDF
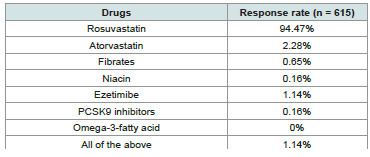 Table 1:Distribution of responses to the preferred lipid-lowering agents in
patients with hyperlipidemia and comorbid hypertension or diabetes
Table 1:Distribution of responses to the preferred lipid-lowering agents in
patients with hyperlipidemia and comorbid hypertension or diabetes
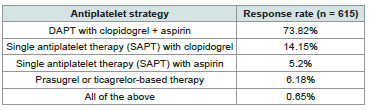 Table 2:Distribution of responses on the preferred initial antiplatelet strategy
post- ACS
Table 2:Distribution of responses on the preferred initial antiplatelet strategy
post- ACS
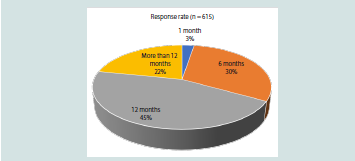 Figure 1:Distribution of responses on the duration of dual antiplatelet therapy
(clopidogrel + aspirin) following PCI with stent placement
Figure 1:Distribution of responses on the duration of dual antiplatelet therapy
(clopidogrel + aspirin) following PCI with stent placement
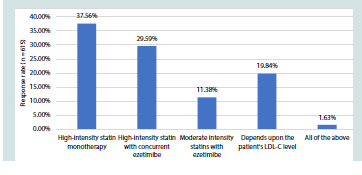 Figure 2:Distribution of responses to the lipid management strategy that was
often preferred in post-ACS patients in your practice
Figure 2:Distribution of responses to the lipid management strategy that was
often preferred in post-ACS patients in your practice
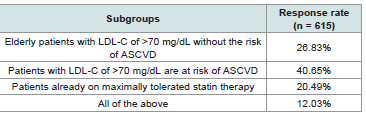 Table 3:Distribution of responses on the clinician-reported subgroups for
recommending rosuvastatin-ezetimibe combination therapy
Table 3:Distribution of responses on the clinician-reported subgroups for
recommending rosuvastatin-ezetimibe combination therapy
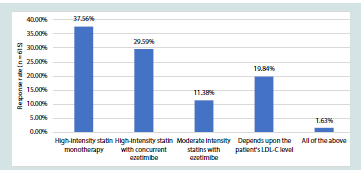 Figure 3: Distribution of responses on the most preferred therapy for a highrisk
patient (ACS + diabetes)
Figure 3: Distribution of responses on the most preferred therapy for a highrisk
patient (ACS + diabetes)
Research Article
Clinician Perspectives on Lipid Management and Antiplatelet Strategies in Acute Coronary Syndrome with A Special Focus On Rosuvastatin in Indian Settings
Manjula S* and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Address for Correspondence:Dr Manjula S, Department of Medical Services, Micro Labs Limited,
Bangalore, Karnataka. E-mail Id: drmanjulas@gmail.com
Submission: 16 April, 2026
Accepted: 06 May, 2026
Published: 08 May, 2026
Copyright: © 2026 Manjula S, et al. This is an open access article
distributed under the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the
original work is properly cited.
Keywords:Acute coronary syndrome; Rosuvastatin; Dual antiplatelet therapy; Lipidlowering
therapy
Abstract
Objective: To assess clinician perspectives and preferences regarding lipid
management and antiplatelet strategies in patients with acute coronary syndrome
(ACS).
Methodology: In this cross-sectional study, a 22-item, multiple-response questionnaire was utilized to gather clinicians’ opinions on current practices, clinical observations, and experiences regarding lipid-lowering and antiplatelet strategies in the routine management of ACS. Data was analyzed using descriptive statistics, with categorical variables presented as percentages and visualized through pie and bar charts in Excel.
Results: The survey included 615 respondents. The majority of clinicians (94.47%) reported prescribing rosuvastatin as the preferred lipid-lowering agent for patients with hyperlipidemia and comorbid hypertension or diabetes. About 74% of the experts favored dual antiplatelet therapy (DAPT) with clopidogrel plus aspirin as the initial antiplatelet strategy for ACS. Approximately 45% opined that DAPT (clopidogrel plus aspirin) is typically continued for 12 months in patients who have undergone percutaneous coronary intervention (PCI) with stent placement. Highintensity statin monotherapy was reported by 38% of participants as the preferred lipid management strategy in post-ACS patients. Approximately 37% of respondents stated that rosuvastatin monotherapy was their preferred approach for high-risk patients (ACS with diabetes), while 36% reported rosuvastatin plus ezetimibe as the preferred choice. Additionally, 41% of experts indicated that the combination of rosuvastatin and ezetimibe is often recommended for patients with LDL-C >70 mg/dL and high atherosclerotic cardiovascular disease (ASCVD) risk.
Conclusion: This study highlights a strong preference for rosuvastatin-centered lipid management and clopidogrel-based DAPT among Indian clinicians treating ACS. High-intensity statin therapy and 12-month DAPT following PCI emerge as common practice patterns. Combination therapy with rosuvastatin and ezetimibe is frequently recommended for patients with elevated LDL-C and high ASCVD risk
Methodology: In this cross-sectional study, a 22-item, multiple-response questionnaire was utilized to gather clinicians’ opinions on current practices, clinical observations, and experiences regarding lipid-lowering and antiplatelet strategies in the routine management of ACS. Data was analyzed using descriptive statistics, with categorical variables presented as percentages and visualized through pie and bar charts in Excel.
Results: The survey included 615 respondents. The majority of clinicians (94.47%) reported prescribing rosuvastatin as the preferred lipid-lowering agent for patients with hyperlipidemia and comorbid hypertension or diabetes. About 74% of the experts favored dual antiplatelet therapy (DAPT) with clopidogrel plus aspirin as the initial antiplatelet strategy for ACS. Approximately 45% opined that DAPT (clopidogrel plus aspirin) is typically continued for 12 months in patients who have undergone percutaneous coronary intervention (PCI) with stent placement. Highintensity statin monotherapy was reported by 38% of participants as the preferred lipid management strategy in post-ACS patients. Approximately 37% of respondents stated that rosuvastatin monotherapy was their preferred approach for high-risk patients (ACS with diabetes), while 36% reported rosuvastatin plus ezetimibe as the preferred choice. Additionally, 41% of experts indicated that the combination of rosuvastatin and ezetimibe is often recommended for patients with LDL-C >70 mg/dL and high atherosclerotic cardiovascular disease (ASCVD) risk.
Conclusion: This study highlights a strong preference for rosuvastatin-centered lipid management and clopidogrel-based DAPT among Indian clinicians treating ACS. High-intensity statin therapy and 12-month DAPT following PCI emerge as common practice patterns. Combination therapy with rosuvastatin and ezetimibe is frequently recommended for patients with elevated LDL-C and high ASCVD risk
Introduction
Acute coronary syndrome (ACS), encompassing ST-segment
elevation myocardial infarction (STEMI) and non-ST-segment
elevation myocardial infarction (NSTEMI), remains a major global
cause of morbidity and mortality.[1] More than 7 million individuals
are diagnosed annually, and ACS constitutes a substantial proportion
of the 17.9 million cardiovascular deaths reported worldwide each year.
[2] ACS accounts for nearly one-third of all deaths among individuals
aged >35 years, underscoring its significant public health impact.
[1] The burden is particularly pronounced in developing countries,
including India, where patients frequently present at a younger age
and with a high prevalence of cardiometabolic comorbidities. India
reports a high proportion of STEMI presentations among ACS cases.
[3,4]
The pathophysiology of ACS is driven by atherosclerotic plaque
rupture and thrombus formation, processes influenced by multiple
modifiable cardiovascular risk factors such as hypertension, diabetes
mellitus, smoking, and dyslipidemia. [1] Among these, dyslipidemia
plays a central role in both the initiation and progression of
atherosclerosis and remains a critical therapeutic target in secondary
prevention. Persistent elevation of low-density lipoprotein cholesterol
(LDL-C) following an index ACS event is strongly associated with
recurrent ischemic events, reinforcing the importance of intensive
lipid-lowering therapy. [5,6]
Recent guidelines strongly recommend early initiation of highintensity statin therapy in patients with ACS to achieve aggressive LDL-C reduction. [6,7] Rosuvastatin is widely used due to its potent LDL-C-lowering capacity, although other high-intensity statins remain guideline-recommended alternatives. Evidence from large clinical trials has demonstrated its effectiveness in achieving substantial lipid reduction and in lowering the risk of subsequent cardiovascular events, supporting its use in high-risk populations. [8-10] In patients who do not achieve recommended lipid targets with statin monotherapy, combination therapy with ezetimibe is advised to reduce residual cardiovascular risk further.[11]
Recent guidelines strongly recommend early initiation of highintensity statin therapy in patients with ACS to achieve aggressive LDL-C reduction. [6,7] Rosuvastatin is widely used due to its potent LDL-C-lowering capacity, although other high-intensity statins remain guideline-recommended alternatives. Evidence from large clinical trials has demonstrated its effectiveness in achieving substantial lipid reduction and in lowering the risk of subsequent cardiovascular events, supporting its use in high-risk populations. [8-10] In patients who do not achieve recommended lipid targets with statin monotherapy, combination therapy with ezetimibe is advised to reduce residual cardiovascular risk further.[11]
Alongside lipid-lowering therapy, dual antiplatelet therapy
(DAPT), typically comprising aspirin and a P2Y12 inhibitor
such as clopidogrel, remains fundamental to ACS management,
particularly after percutaneous coronary intervention (PCI) with
stent implantation. The duration of DAPT and subsequent long-term
antiplatelet strategies requires careful individualization based on the
patient’s ischemic and bleeding risks. [12]
Although international guidelines provide clear recommendations for lipid-lowering and antiplatelet therapy in ACS, [13] understanding expert perspectives and preferences is important to identify prevailing trends and areas of consensus in contemporary clinical practice. The present study aims to assess expert perspectives on rosuvastatin centered lipid management and antiplatelet strategies in patients with ACS, with particular emphasis on treatment preferences, duration of DAPT, lipid-lowering combinations, and achievement of dyslipidemia goals in routine practice.
Although international guidelines provide clear recommendations for lipid-lowering and antiplatelet therapy in ACS, [13] understanding expert perspectives and preferences is important to identify prevailing trends and areas of consensus in contemporary clinical practice. The present study aims to assess expert perspectives on rosuvastatin centered lipid management and antiplatelet strategies in patients with ACS, with particular emphasis on treatment preferences, duration of DAPT, lipid-lowering combinations, and achievement of dyslipidemia goals in routine practice.
Methodology
A cross-sectional study was carried out among clinicians
specialized in managing ACS in the major Indian cities from June
2025 to December 2025.
Questionnaire:
The questionnaire booklet titled HEARTLINE (Healthcare
Experts’ Assessment on Rosuvastatin in Dyslipidemia Management)
study was sent to the doctors who were interested in participating
in this study. A 23-item structured, multiple-response questionnaire
aimed to capture clinical perspectives on lipid-lowering and
antiplatelet strategies in ACS, with a specific focus on Rosuvastatin
and its combinations. The study was performed after obtaining
approval from Bangalore Ethics, an Independent Ethics Committee,
which was recognized by the Indian Regulatory Authority, the Drug
Controller General of India.
Participants:
An invitation was sent to professionals across India based
on their expertise and experience in treating ACS in the month
of March 2025 for participation in this Indian survey. About 615
clinicians from major cities of all Indian states, representing the
geographical distribution, shared their willingness to participate and
provide necessary data. Clinicians were instructed to complete the
questionnaire independently without consulting colleagues. Written
informed consent was obtained from each participant before the
study began.
Statistical analysis:
Data were analyzed using descriptive statistical methods.
Categorical variables are presented as frequencies and percentages
to illustrate their distribution. The occurrence and proportional
representation of each response category were calculated. Graphical
representations were generated to visually depict response
distributions using Microsoft Excel (version 16.0.18025.20030).
Results
The study included 615 experts, of whom 40% reported that
41–50% of their ACS patients are aged >40-60 years. More than half
(51.54%) of clinicians reported that 21–30% of their patients have
comorbid hyperlipidemia and hypertension. Similarly, 52% stated
that 21–30% of patients have comorbid hyperlipidemia and diabetes.
According to 54% of clinicians, the highest prevalence of ACS
was observed among male patients, whereas 43% reported no gender
difference. Approximately 49% of respondents reported prescribing
statins as add-on therapy for primary prevention in 30–40% of
patients with dyslipidemia, while 42% indicated prescribing them in
20-30% of such patients.
The majority of clinicians (94.47%) reported prescribing
rosuvastatin as the preferred lipid-lowering agent for patients with
hyperlipidemia and comorbid hypertension or diabetes [Table 1].
More than half (64.07%) reported that the preferred dose of
rosuvastatin in patients with diabetes, irrespective of lipid levels,
was 10 mg. About 74% of the experts indicated that DAPT with
clopidogrel + aspirin was the preferred initial antiplatelet strategy for
ACS [Table 2].
More than half (53.82%) of the participants reported that 20
to 30% of the patients would require DAPT + statin treatment.
Approximately 45% of the participants opined that dual antiplatelet
therapy (clopidogrel + aspirin) is typically continued for 12 months
in patients who have undergone PCI with stent placement
[Figure 1]. About 42% of clinicians stated that the preferred strategy for
long-term secondary prevention after an ACS event, following
completion of DAPT, is continuation of single antiplatelet therapy
(SAPT) with clopidogrel. Nearly half of the clinicians (50.57%)
reported that in patients with a prior stroke and high ischemic risk,
DAPT is recommended for approximately 12 months or longer.
Around 36% of participants opined that dual antiplatelet therapy
is extended beyond 12 months in post–myocardial infarction (MI)
patients with high ischemic and low bleeding risk, but only in
selected high-risk individuals. As reported by 62% of respondents, the
preferred antiplatelet strategy after coronary artery bypass grafting
(CABG) in ACS patients was DAPT for 12 months followed by SAPT.
Additionally, 38% of participants reported that high-intensity statin
monotherapy was the preferred lipid management strategy in post-
ACS patients [Figure 2].
As reported by 30% of respondents, approximately 50–60% of
patients with ACS receive high-intensity statin therapy despite having
LDL-C levels >70 mg/dL. Nearly 39% of participants stated that they
recommend a fasting lipid panel for patients approximately 3 months
after discharge following ACS.
As indicated by 41% of experts, patients with LDL-C >70 mg/dL and a risk of ASCVD are often recommended combination therapy with rosuvastatin and ezetimibe (Table 3). A significant proportion (76.42%) of clinicians reported not observing any adverse reactions in patients receiving rosuvastatin. Additionally, about 64% of clinicians reported marked improvement in achieving dyslipidemia goals with rosuvastatin, based on the 5-point global improvement scale. According to 37% of respondents, rosuvastatin monotherapy was the most preferred approach for high-risk patients (ACS with diabetes), while 36% reported rosuvastatin plus ezetimibe as the preferred choice [Figure 3]. Over 37% of clinicians reported that the perceived advantages associated with the initiation of rosuvastatin along with DAPT include superior LDL-C reduction, and potential reductions in recurrent ischemic stroke, major adverse cardiovascular events (MACE), and overall mortality.
As indicated by 41% of experts, patients with LDL-C >70 mg/dL and a risk of ASCVD are often recommended combination therapy with rosuvastatin and ezetimibe (Table 3). A significant proportion (76.42%) of clinicians reported not observing any adverse reactions in patients receiving rosuvastatin. Additionally, about 64% of clinicians reported marked improvement in achieving dyslipidemia goals with rosuvastatin, based on the 5-point global improvement scale. According to 37% of respondents, rosuvastatin monotherapy was the most preferred approach for high-risk patients (ACS with diabetes), while 36% reported rosuvastatin plus ezetimibe as the preferred choice [Figure 3]. Over 37% of clinicians reported that the perceived advantages associated with the initiation of rosuvastatin along with DAPT include superior LDL-C reduction, and potential reductions in recurrent ischemic stroke, major adverse cardiovascular events (MACE), and overall mortality.
Discussion
The findings of the current study demonstrate a substantial
burden of cardiometabolic comorbidities among patients with ACS
and reflect a clear shift toward guideline-aligned, risk-stratified,
and rosuvastatin-centered management strategies in routine Indian
clinical practice. A large proportion of clinicians reported preferring
rosuvastatin as the primary lipid-lowering agent in patients
with hyperlipidemia and coexisting hypertension or diabetes,
highlighting its perceived efficacy across high-risk subgroups. The
observed preference for rosuvastatin in the present survey should be
interpreted with caution. This finding may be influenced by several
factors, including cost, drug availability, clinician familiarity, and
market presence in India. Recent international guidelines from
professional bodies recommend high-intensity statin therapy as a
class effect rather than favoring a specific molecule. [7] Therefore,
the lower reported use of alternatives such as atorvastatin and newer
lipid-lowering agents in this survey likely reflects differences in
access, affordability, and prescribing practices rather than differences
in clinical efficacy. A similar contextual interpretation applies to
antiplatelet therapy. Although ticagrelor and prasugrel are guideline preferred
P2Y12 inhibitors in many ACS settings, the continued
predominance of clopidogrel observed in this study may be attributed
to cost considerations, concerns regarding bleeding risk, and wider
availability in routine Indian clinical practice.
In addition, these observations are consistent with previously
published evidence. Rani et al. reported that rosuvastatin therapy
significantly reduced LDL cholesterol levels over a 12-week treatment
period.[9] Aggarwal and Show kathali concluded that rosuvastatin
is considered a potent statin with established efficacy and safety in
patients with ACS.[14] Similarly, McKenney JM demonstrated that
rosuvastatin has been shown in comparative studies to be more
effective in lowering LDL-C and non-HDL cholesterol concentrations
compared with other statins in the management of dyslipidemia.
[15] Barakat et al. further showed that rosuvastatin 10 mg has
been reported as one of the more effective statin doses for LDL-C
reduction.[10]
The present survey also indicates that DAPT with clopidogrel plus aspirin remains the preferred initial antiplatelet strategy in ACS. This finding was consistent with Sawhney et al., who observed that DAPT with clopidogrel and aspirin was the predominant discharge strategy for ACS in India, with 78.8% of patients discharged on DAPT and more than half continuing therapy at 2-year follow-up.[16] These findings reinforce that contemporary prescribing patterns in India are broadly aligned with real-world evidence and established clinical data supporting the established role of DAPT as a cornerstone of ACS management. The INDEPTH survey conducted by Hiremath et al. also reported that DAPT with clopidogrel plus aspirin is the preferred initial antiplatelet strategy for ACS, often used as part of triple-drug therapy with a statin. The study further noted that most interventional cardiologists recommend maintaining DAPT for 6 to 12 months or even longer after ACS. [17] Similarly, Mohan et al. demonstrated widespread use of clopidogrel-based DAPT in post-PCI patients, reporting that more than 90% of patients with coronary artery disease (CAD) received DAPT after PCI, with continuation for up to one year in routine clinical practice.[18] These findings are consistent with the current survey, which indicates continuation of DAPT for 12 months following PCI with stent implantation.
The present survey also indicates that DAPT with clopidogrel plus aspirin remains the preferred initial antiplatelet strategy in ACS. This finding was consistent with Sawhney et al., who observed that DAPT with clopidogrel and aspirin was the predominant discharge strategy for ACS in India, with 78.8% of patients discharged on DAPT and more than half continuing therapy at 2-year follow-up.[16] These findings reinforce that contemporary prescribing patterns in India are broadly aligned with real-world evidence and established clinical data supporting the established role of DAPT as a cornerstone of ACS management. The INDEPTH survey conducted by Hiremath et al. also reported that DAPT with clopidogrel plus aspirin is the preferred initial antiplatelet strategy for ACS, often used as part of triple-drug therapy with a statin. The study further noted that most interventional cardiologists recommend maintaining DAPT for 6 to 12 months or even longer after ACS. [17] Similarly, Mohan et al. demonstrated widespread use of clopidogrel-based DAPT in post-PCI patients, reporting that more than 90% of patients with coronary artery disease (CAD) received DAPT after PCI, with continuation for up to one year in routine clinical practice.[18] These findings are consistent with the current survey, which indicates continuation of DAPT for 12 months following PCI with stent implantation.
The present survey found that high-intensity statin monotherapy
remains the preferred lipid-lowering strategy in patients following
ACS, suggesting alignment with contemporary guideline
recommendations that advocate early and sustained intensive LDL-C
reduction for secondary prevention. This observation was consistent
with findings from Mahajan et al., who reported that 73.1% of patients
with established coronary artery disease, including those with prior
ACS, were prescribed high-intensity statins.[19] Similarly, Jain et
al. noted that the majority of ACS patients received high-intensity
statin therapy as a part of routine post-ACS management.[20] Nayak
et al. further demonstrated that 81.8% of post-ACS patients in India
were treated with high-intensity statin monotherapy for secondary
prevention, underscoring the widespread uptake of this strategy in
clinical practice.[21] Together, these studies reinforce the central role
of high-intensity statins as the cornerstone of lipid management after
ACS.
The current survey also identified rosuvastatin monotherapy as the most preferred lipid-lowering approach in high-risk patients with ACS and concomitant diabetes, with a considerable proportion of clinicians additionally favoring combination therapy with rosuvastatin and ezetimibe. This preference likely reflects the potent LDL-C– lowering efficacy and favorable tolerability profile of rosuvastatin, particularly in high-risk metabolic populations. Supporting this trend, Dadzie et al. reported that rosuvastatin, administered either as monotherapy or in combination with ezetimibe, has been shown to achieve significant lipid reductions in patients with type 2 diabetes.[22] Likewise, Ballantyne et al. demonstrated that although rosuvastatin monotherapy produces substantial LDL-C lowering in high-risk individuals, the addition of ezetimibe has been shown to significantly improve LDL-C goal attainment rates.[23] Furthermore, Halatiu et al. observed that the rosuvastatin–ezetimibe combination has been associated with a greater proportion of ACS patients achieving recommended LDL-C targets compared with statin monotherapy alone.[24] Studies have also shown that combining rosuvastatin and ezetimibe is a highly effective, well-tolerated, and frequently recommended strategy for patients with ASCVD and LDL-C >70 mg/dL, often achieving LDL-C reduction.[25,26]Similar results were also observed in the present study, with LDL-C >70 mg/ dL, where the risk of ASCVD often recommended the combination of rosuvastatin and ezetimibe.
In the current survey, a significant proportion of clinicians reported that they had not observed any notable ADRs in patients receiving rosuvastatin, supporting clinicians’ perceptions of its safety and tolerability in routine clinical practice. This favorable safety profile is particularly relevant in post-ACS settings, where long-term adherence to high-intensity statin therapy is critical for sustained cardiovascular risk reduction. These findings are supported by published evidence. Shah et al. evaluated intensive rosuvastatin therapy (40 mg/day) in patients with ACS and reported that the regimen has been reported to be effective and well tolerated. Only a small proportion of patients experienced minor adverse events, such as myalgia, and no serious ADRs or clinically significant laboratory abnormalities were documented.[27] Similarly, Tan et al. reported a
The current survey also identified rosuvastatin monotherapy as the most preferred lipid-lowering approach in high-risk patients with ACS and concomitant diabetes, with a considerable proportion of clinicians additionally favoring combination therapy with rosuvastatin and ezetimibe. This preference likely reflects the potent LDL-C– lowering efficacy and favorable tolerability profile of rosuvastatin, particularly in high-risk metabolic populations. Supporting this trend, Dadzie et al. reported that rosuvastatin, administered either as monotherapy or in combination with ezetimibe, has been shown to achieve significant lipid reductions in patients with type 2 diabetes.[22] Likewise, Ballantyne et al. demonstrated that although rosuvastatin monotherapy produces substantial LDL-C lowering in high-risk individuals, the addition of ezetimibe has been shown to significantly improve LDL-C goal attainment rates.[23] Furthermore, Halatiu et al. observed that the rosuvastatin–ezetimibe combination has been associated with a greater proportion of ACS patients achieving recommended LDL-C targets compared with statin monotherapy alone.[24] Studies have also shown that combining rosuvastatin and ezetimibe is a highly effective, well-tolerated, and frequently recommended strategy for patients with ASCVD and LDL-C >70 mg/dL, often achieving LDL-C reduction.[25,26]Similar results were also observed in the present study, with LDL-C >70 mg/ dL, where the risk of ASCVD often recommended the combination of rosuvastatin and ezetimibe.
In the current survey, a significant proportion of clinicians reported that they had not observed any notable ADRs in patients receiving rosuvastatin, supporting clinicians’ perceptions of its safety and tolerability in routine clinical practice. This favorable safety profile is particularly relevant in post-ACS settings, where long-term adherence to high-intensity statin therapy is critical for sustained cardiovascular risk reduction. These findings are supported by published evidence. Shah et al. evaluated intensive rosuvastatin therapy (40 mg/day) in patients with ACS and reported that the regimen has been reported to be effective and well tolerated. Only a small proportion of patients experienced minor adverse events, such as myalgia, and no serious ADRs or clinically significant laboratory abnormalities were documented.[27] Similarly, Tan et al. reported a
low incidence of significant ADRs with rosuvastatin therapy, further
reinforcing its safety profile.[28] In addition, Rahhal et al. compared
high-intensity rosuvastatin with high-intensity atorvastatin in
ACS patients and found comparable safety outcomes between
the two agents, with no increase in adverse events associated with
rosuvastatin.[29] This suggests that rosuvastatin offers a safety profile
similar to other high-intensity statins while maintaining robust lipid lowering
efficacy.
A key strength of the present survey is its large sample size of cardiologists and physicians across diverse clinical settings in India, providing broader insights into contemporary ACS management practices. The use of a structured 22-item questionnaire comprehensively captured lipid-lowering strategies, enabling a holistic understanding of post-ACS care. The focus on high-risk subgroups, including patients with diabetes, prior stroke, post-PCI, and post-CABG, further enhances its clinical relevance. However, the cross-sectional design limits causal inference and captures practices at only a single time point. Reliance on self-reported responses introduces the potential for recall and social desirability bias, and the absence of patient-level clinical or outcome data precludes correlation between reported practices and actual cardiovascular outcomes. As the survey reflects practices within India, generalizability to other healthcare settings may be limited. Despite these constraints, the study provides valuable insights into current lipid and antiplatelet management patterns in ACS.
A key strength of the present survey is its large sample size of cardiologists and physicians across diverse clinical settings in India, providing broader insights into contemporary ACS management practices. The use of a structured 22-item questionnaire comprehensively captured lipid-lowering strategies, enabling a holistic understanding of post-ACS care. The focus on high-risk subgroups, including patients with diabetes, prior stroke, post-PCI, and post-CABG, further enhances its clinical relevance. However, the cross-sectional design limits causal inference and captures practices at only a single time point. Reliance on self-reported responses introduces the potential for recall and social desirability bias, and the absence of patient-level clinical or outcome data precludes correlation between reported practices and actual cardiovascular outcomes. As the survey reflects practices within India, generalizability to other healthcare settings may be limited. Despite these constraints, the study provides valuable insights into current lipid and antiplatelet management patterns in ACS.
Conclusion
This study highlights clinician-reported preferences for
rosuvastatin-centered lipid management and clopidogrel-based
dual antiplatelet therapy in ACS across Indian practice settings.
These findings reflect prevailing treatment perceptions rather than
outcome-based evidence and should be interpreted in the context of
survey-based limitations.
Acknowledgement
We would like to thank all the clinicians who participated in this
study.
Conflict of Interest:
The authors are employees of Micro Labs Limited. The study was
designed and conducted as part of a scientific initiative. The authors
declare that no undue influence was exerted on data collection,
analysis, or interpretation.
Funding:
This study was funded by Micro Labs Limited. The sponsor had
a role in study conceptualization and questionnaire development but
did not influence the interpretation of results.
References
Citation
Manjula S, Krishna Kumar M. Clinician Perspectives on Lipid Management and Antiplatelet Strategies in Acute Coronary Syndrome with A Special Focus On Rosuvastatin in Indian Settings. J Cardiobiol. 2026;10(1): 1.