
Journal of Cardiobiology
Download PDF
Heart sounds primarily originate from vibrations produced during cardiac valve closure and blood flow turbulence. The two fundamental heart sounds are:
• First heart sound (S1): produced by closure of the atrioventricular valves.
• Second heart sound (S2): produced by closure of the semilunar valves.
Additional sounds such as S3 and S4, as well as systolic and diastolic murmurs, can also be recorded using PCG.
The phonocardiogram is usually synchronized with an electrocardiographic (ECG) tracing to correlate acoustic events with electrical cardiac activity.
• Digital recording of heart sounds
• Noise filtering
• Waveform visualization
• Storage and remote sharing of recordings
These innovations have facilitated the integration of PCG into routine clinical practice.
PCG provides an objective method to document systolic and diastolic murmurs. It allows clinicians to determine:
• Timing of murmurs
• Intensity
• Duration
• Frequency characteristics
This is particularly useful for differentiating pathological murmurs from innocent murmurs in clinical settings.
Phonocardiography features:
• Harsh crescendo–decrescendo systolic murmur
• Begins shortly after S1 and peaks in mid-systole
• Terminates before S2
• Often associated with reduced or delayed A2 component of S2
• Possible ejection clicks in congenital cases
Phonocardiography features:
• High-pitched early diastolic decrescendo murmur
• Begins immediately after A2
• Best recorded along the left sternal border
• May be accompanied by Austin Flint murmur, a mid-diastolic rumble caused by regurgitant jet interference with the mitral valve
• Loud S1 due to stiff valve closure
• Opening snap (OS) shortly after S2
• Low-frequency diastolic rumbling murmur
• Presystolic accentuation in patients with sinus rhythm
• Shorter S2–OS interval correlates with increased severity
• Holosystolic (pansystolic) murmur
• Begins with S1 and extends to S2
• Usually uniform intensity
• Often associated with soft or absent S1
• May show S3 due to volume overload
Phonocardiography features
• Mid-systolic click
• Followed by a late systolic murmur
• Murmur duration varies with ventricular volume
Phonocardiography features
• Holosystolic murmur
• Best heard at the lower left sternal border
• Murmur intensity increases during inspiration (Carvallo’s sign)
• Possible right-sided S3
Phonocardiography features
• Diastolic rumbling murmur
• Occurs after an opening snap
• Intensifies with inspiration
• Associated with prominent jugular venous pulsations
• Best recorded at the left upper sternal border
• May include an ejection click
• Delayed P2 component of S2
Phonocardiography features
• Early diastolic decrescendo murmur
• Best heard at the left upper sternal border
• In pulmonary hypertension, produces the Graham Steell murmur
• Ventricular Septal Defect
• Patent Ductus Arteriosus
• Atrial Septal Defect
Early recognition of abnormal heart sounds may prompt timely referral for definitive imaging.
AI-assisted PCG systems are capable of:
• automated murmur detection
• classification of heart sounds
• prediction of valvular disease
These technologies may improve diagnostic accuracy and reduce dependence on subjective clinical interpretation. Modern PCG analysis systems utilize machine learning algorithms trained on large datasets of annotated heart sound recordings.
Heart sound recordings are first processed to remove background noise using techniques such as:
• band-pass filtering
• wavelet transformation
• adaptive noise cancellation
2. Feature Extraction
Important acoustic features are extracted from the phonocardiogram, including:
• frequency spectrum
• temporal features (S1–S2 intervals)
• amplitude variation
• spectral entropy
3. Machine Learning Models
Extracted features are then analyzed using algorithms such as:
• Convolutional Neural Networks (CNN)
• Recurrent Neural Networks (RNN)
• Vision Transformers
• Support Vector Machines (SVM)
Deep learning models are particularly effective because they can automatically identify complex patterns in heart sound recordings.
AI-assisted PCG systems have demonstrated encouraging results in murmur detection and classification:
• Sensitivity for pathological murmur detection: 80–92%
• Specificity: 75–90%
• Overall classification accuracy: approximately 85–90%
Deep learning models trained on large heart sound datasets have achieved particularly strong performance. In a study published in IEEE Journal of Biomedical and Health Informatics, transformerbased neural networks identified congenital valvular murmurs with an accuracy exceeding 88%.
Similarly, research in Computers in Biology and Medicine reported that AI-assisted PCG could distinguish normal from abnormal heart sounds with over 90% sensitivity in controlled datasets.
Despite these promising findings, real-world diagnostic performance may be lower due to background noise, patient variability, and recording conditions. Consequently, PCG is currently best regarded as a screening or triage tool rather than a definitive diagnostic modality.
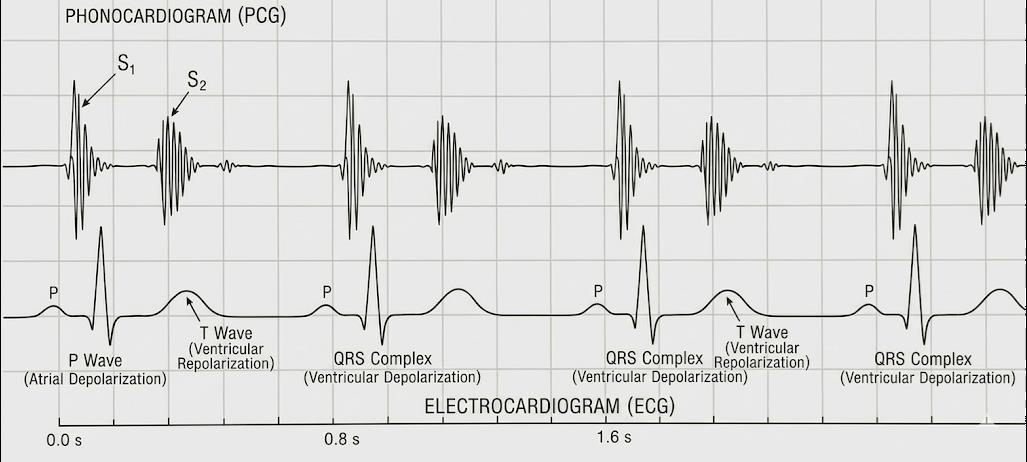 Figure 1:Simultaneous recording of phonocardiography (PCG) and electrocardiography (ECG) demonstrate correlation between electrical and acoustic cardiac events.
Figure 1:Simultaneous recording of phonocardiography (PCG) and electrocardiography (ECG) demonstrate correlation between electrical and acoustic cardiac events.
 Figure 2:Systolic murmurs occur during heart muscle contraction (between
S1 and S2 sounds) due to heart valve stenosis or regurgitation. While
diastolic murmurs (between S2 and S1) are noticed in cases of mitral or
tricuspid stenosis.
Figure 2:Systolic murmurs occur during heart muscle contraction (between
S1 and S2 sounds) due to heart valve stenosis or regurgitation. While
diastolic murmurs (between S2 and S1) are noticed in cases of mitral or
tricuspid stenosis.
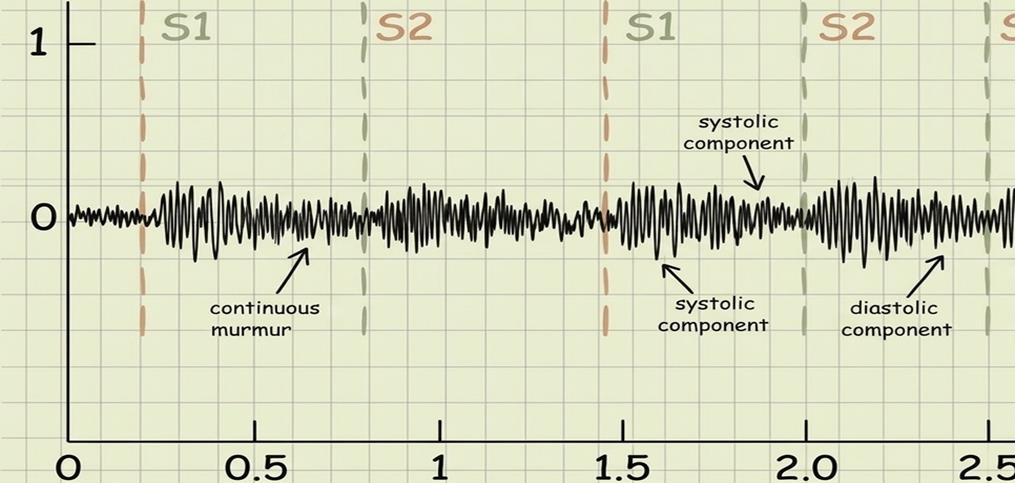 Figure 3:Continuous murmurs are classically associated with Patent Ductus
Arteriosus. Ventricular septal defects typically produce holosystolic murmurs.
Figure 3:Continuous murmurs are classically associated with Patent Ductus
Arteriosus. Ventricular septal defects typically produce holosystolic murmurs.
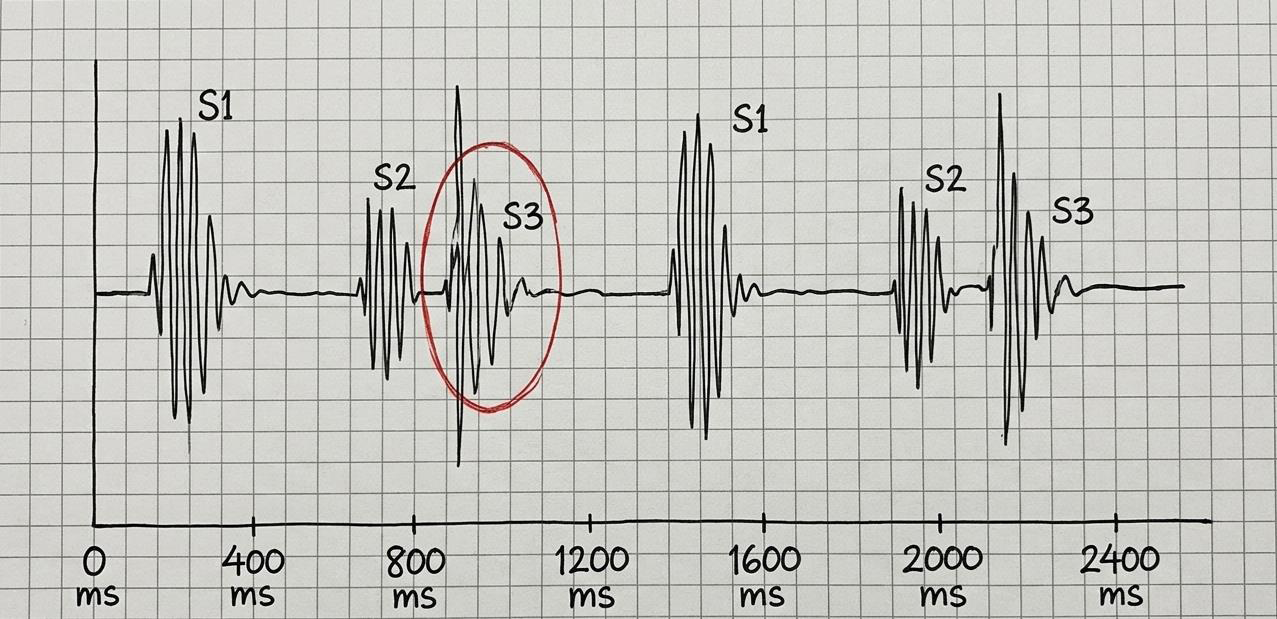 Figure 4:Abnormal S3 which may often indicate systolic heart failure, volume
overload, or mitral regurgitation.
Figure 4:Abnormal S3 which may often indicate systolic heart failure, volume
overload, or mitral regurgitation.
• valve morphology
• chamber dimensions
• ventricular function
• blood flow patterns
Because of these capabilities, echocardiography remains the gold-standard imaging modality. However, PCG offers several complementary advantages:
• Portable and easy to perform
• Suitable for mass screening
• Allows continuous monitoring
• Enables digital storage and telemedicine applications
• Quantitative hemodynamic assessment
• Precise measurement of valve gradients and regurgitation severity
In practical clinical workflows, PCG may be particularly useful for:
• Primary care screening for heart murmurs
• Rural or resource-limited settings where echocardiography is unavailable
• Telemedicine-based cardiac evaluation
• Medical education and auscultation training In such contexts, abnormal PCG findings can serve as a trigger for referral for definitive imaging with echocardiography.
Review Article
Phonocardiography: Revival of Cardiac Auscultation in the Digital Era: A Clinician-Oriented Review
Sibi Das
Department of Medicine NC Medical College and Hospital Israna, Panipat, Haryana, India.
*Address for Correspondence:Dr. Sibi Das, Department of Medicine NC Medical College and Hospital
Israna, Panipat, Haryana, India
Submission: 26 February, 2026
Accepted: 25 March, 2026
Published: 28 March, 2026
Copyright: © 2026 Das S. This is an open access article distributed under
the Creative Commons Attribution License, which permits unrestricted use,
distribution, and reproduction in any medium, provided the original work is
properly cited.
Keywords:Phonocardiography; Cardiac Auscultation; Digital
Stethoscope; Heart Murmurs, Cardiovascular Screening; Artificial
Intelligence
Abstract
Cardiac auscultation remains a fundamental component
of bedside cardiovascular examination. However, traditional
auscultation using an acoustic stethoscope is highly dependent on
clinician expertise and subjective interpretation. Phonocardiography
(PCG), the graphical recording of heart sounds and murmurs, provides
an objective method for analyzing cardiac acoustic signals. With the
emergence of digital stethoscopes, advanced signal processing, and
artificial intelligence (AI)–based sound analysis, PCG has significantly
regained attention as a diagnostic adjunct in contemporary cardiology.
Recent studies have demonstrated promising diagnostic performance of PCG-based algorithms, with reported sensitivities ranging from 80–92% and specificities of 75–90% for detecting pathological heart murmurs and certain valvular heart diseases. While echocardiography remains the gold standard for structural cardiac evaluation, PCG offers advantages in screening, documentation, and remote monitoring, particularly in primary care and resource-limited settings.
This review discusses the principles of phonocardiography, current clinical applications, diagnostic performance, integration with artificial intelligence, and its potential role alongside echocardiography in modern clinical practice.
Recent studies have demonstrated promising diagnostic performance of PCG-based algorithms, with reported sensitivities ranging from 80–92% and specificities of 75–90% for detecting pathological heart murmurs and certain valvular heart diseases. While echocardiography remains the gold standard for structural cardiac evaluation, PCG offers advantages in screening, documentation, and remote monitoring, particularly in primary care and resource-limited settings.
This review discusses the principles of phonocardiography, current clinical applications, diagnostic performance, integration with artificial intelligence, and its potential role alongside echocardiography in modern clinical practice.
Introduction
Cardiac auscultation has been a cornerstone of bedside diagnosis
since the invention of the stethoscope by René Laennec in 1816.
Despite remarkable advances in cardiovascular imaging such
as echocardiography and cardiac magnetic resonance imaging,
auscultation continues to play an essential role in initial cardiovascular
evaluation.
However, conventional auscultation has important limitations. Several studies have demonstrated significant variability in the diagnostic accuracy of cardiac auscultation among clinicians. In a classic study published in JAMA, only 20–40% of trainees were able to correctly identify common cardiac murmurs during auscultation. Phonocardiography (PCG) was introduced to address these limitations by providing an objective visual representation of heart sounds. Early PCG systems gained popularity during the mid-20th century but were gradually replaced by echocardiography due to the latter’s ability to visualize cardiac anatomy directly.
In recent years, the development of digital stethoscopes, advanced signal processing, and machine learning–based acoustic analysis has renewed interest in PCG. Contemporary PCG systems can detect abnormal heart sounds with diagnostic accuracies approaching those of expert clinicians, making them potentially valuable tools for cardiovascular screening and education.
However, conventional auscultation has important limitations. Several studies have demonstrated significant variability in the diagnostic accuracy of cardiac auscultation among clinicians. In a classic study published in JAMA, only 20–40% of trainees were able to correctly identify common cardiac murmurs during auscultation. Phonocardiography (PCG) was introduced to address these limitations by providing an objective visual representation of heart sounds. Early PCG systems gained popularity during the mid-20th century but were gradually replaced by echocardiography due to the latter’s ability to visualize cardiac anatomy directly.
In recent years, the development of digital stethoscopes, advanced signal processing, and machine learning–based acoustic analysis has renewed interest in PCG. Contemporary PCG systems can detect abnormal heart sounds with diagnostic accuracies approaching those of expert clinicians, making them potentially valuable tools for cardiovascular screening and education.
Principles of Phonocardiography:
Phonocardiography refers to the recording of heart sounds and
murmurs using sensitive microphones or electronic sensors placed
on the chest wall. These sounds are converted into electrical signals
and displayed graphically as waveforms.Heart sounds primarily originate from vibrations produced during cardiac valve closure and blood flow turbulence. The two fundamental heart sounds are:
• First heart sound (S1): produced by closure of the atrioventricular valves.
• Second heart sound (S2): produced by closure of the semilunar valves.
Additional sounds such as S3 and S4, as well as systolic and diastolic murmurs, can also be recorded using PCG.
The phonocardiogram is usually synchronized with an electrocardiographic (ECG) tracing to correlate acoustic events with electrical cardiac activity.
Evolution of Phonocardiography:
Early phonocardiography systems were bulky and required
specialized equipment. As a result, their use remained largely confined
to research laboratories. The advent of portable electronic sensors and
digital stethoscopes has significantly simplified the recording process.
Modern PCG systems allow:• Digital recording of heart sounds
• Noise filtering
• Waveform visualization
• Storage and remote sharing of recordings
These innovations have facilitated the integration of PCG into routine clinical practice.
Clinical Applications of Phonocardiography:
1. Detection of Heart MurmursPCG provides an objective method to document systolic and diastolic murmurs. It allows clinicians to determine:
• Timing of murmurs
• Intensity
• Duration
• Frequency characteristics
This is particularly useful for differentiating pathological murmurs from innocent murmurs in clinical settings.
2. Valvular Heart Disease:
Phonocardiography plays a significant role in the evaluation of
valvular disorders. Characteristic phonocardiography patterns help
identify the timing and acoustic features of murmurs associated with
these conditions. While echocardiography remains the gold standard
for diagnosis, PCG can serve as a useful screening tool.
Aortic Stenosis:
Aortic stenosis results from obstruction to left ventricular
outflow due to narrowing of the aortic valve. Common causes include
degenerative calcification, congenital bicuspid valve, and rheumatic
disease.Phonocardiography features:
• Harsh crescendo–decrescendo systolic murmur
• Begins shortly after S1 and peaks in mid-systole
• Terminates before S2
• Often associated with reduced or delayed A2 component of S2
• Possible ejection clicks in congenital cases
Aortic Regurgitation:
Aortic regurgitation occurs when the aortic valve fails to close
completely, allowing retrograde blood flow into the left ventricle
during diastole.Phonocardiography features:
• High-pitched early diastolic decrescendo murmur
• Begins immediately after A2
• Best recorded along the left sternal border
• May be accompanied by Austin Flint murmur, a mid-diastolic rumble caused by regurgitant jet interference with the mitral valve
Mitral Stenosis:
Mitral stenosis is most caused by rheumatic heart disease, leading
to obstruction of blood flow from the left atrium to the left ventricle.
Phonocardiography features• Loud S1 due to stiff valve closure
• Opening snap (OS) shortly after S2
• Low-frequency diastolic rumbling murmur
• Presystolic accentuation in patients with sinus rhythm
• Shorter S2–OS interval correlates with increased severity
Mitral Regurgitation:
Mitral regurgitation occurs when the mitral valve fails to close
properly during systole, allowing backward flow into the left atrium.
Phonocardiography features:• Holosystolic (pansystolic) murmur
• Begins with S1 and extends to S2
• Usually uniform intensity
• Often associated with soft or absent S1
• May show S3 due to volume overload
Mitral Valve Prolapse:
Mitral valve prolapses results from systolic displacement of the
mitral leaflets into the left atrium.Phonocardiography features
• Mid-systolic click
• Followed by a late systolic murmur
• Murmur duration varies with ventricular volume
Tricuspid Regurgitation:
Tricuspid regurgitation involves backflow of blood from the right
ventricle to the right atrium during systole.Phonocardiography features
• Holosystolic murmur
• Best heard at the lower left sternal border
• Murmur intensity increases during inspiration (Carvallo’s sign)
• Possible right-sided S3
Tricuspid Stenosis:
Tricuspid stenosis is a relatively rare condition, most commonly
of rheumatic origin.Phonocardiography features
• Diastolic rumbling murmur
• Occurs after an opening snap
• Intensifies with inspiration
• Associated with prominent jugular venous pulsations
Pulmonary Stenosis:
Pulmonary stenosis is commonly congenital, leading to
obstruction of right ventricular outflow.
Phonocardiography features:
• Systolic crescendo–decrescendo murmur• Best recorded at the left upper sternal border
• May include an ejection click
• Delayed P2 component of S2
Pulmonary Regurgitation:
Pulmonary regurgitation occurs when the pulmonary valve fails
to close completely.Phonocardiography features
• Early diastolic decrescendo murmur
• Best heard at the left upper sternal border
• In pulmonary hypertension, produces the Graham Steell murmur
3. Congenital Heart Disease:
Phonocardiography can assist in the early detection of congenital
cardiac anomalies, including:• Ventricular Septal Defect
• Patent Ductus Arteriosus
• Atrial Septal Defect
Early recognition of abnormal heart sounds may prompt timely referral for definitive imaging.
4. Heart Failure Evaluation:
The presence of a third heart sound (S3) is commonly associated
with ventricular dysfunction and volume overload, particularly in
patients with systolic heart failure. PCG can detect low-frequency
sounds that may be difficult to appreciate with conventional
auscultation.
5. Cardiovascular Screening:
In primary care and community health settings, PCG may serve
as a cost-effective screening tool for cardiovascular disease, especially
in regions where access to advanced imaging is limited.
Integration with Artificial Intelligence:
Recent advances in machine learning have significantly expanded
the diagnostic potential of phonocardiography. Artificial intelligence
algorithms can analyze large datasets of heart sound recordings to
detect abnormal patterns.AI-assisted PCG systems are capable of:
• automated murmur detection
• classification of heart sounds
• prediction of valvular disease
These technologies may improve diagnostic accuracy and reduce dependence on subjective clinical interpretation. Modern PCG analysis systems utilize machine learning algorithms trained on large datasets of annotated heart sound recordings.
Common methodologies include::
1. Signal Processing TechniquesHeart sound recordings are first processed to remove background noise using techniques such as:
• band-pass filtering
• wavelet transformation
• adaptive noise cancellation
2. Feature Extraction
Important acoustic features are extracted from the phonocardiogram, including:
• frequency spectrum
• temporal features (S1–S2 intervals)
• amplitude variation
• spectral entropy
3. Machine Learning Models
Extracted features are then analyzed using algorithms such as:
• Convolutional Neural Networks (CNN)
• Recurrent Neural Networks (RNN)
• Vision Transformers
• Support Vector Machines (SVM)
Deep learning models are particularly effective because they can automatically identify complex patterns in heart sound recordings.
Diagnostic Accuracy and Quantitative Evidence:
Several recent studies have evaluated the diagnostic performance
of AI-assisted phonocardiography systems.AI-assisted PCG systems have demonstrated encouraging results in murmur detection and classification:
• Sensitivity for pathological murmur detection: 80–92%
• Specificity: 75–90%
• Overall classification accuracy: approximately 85–90%
Deep learning models trained on large heart sound datasets have achieved particularly strong performance. In a study published in IEEE Journal of Biomedical and Health Informatics, transformerbased neural networks identified congenital valvular murmurs with an accuracy exceeding 88%.
Similarly, research in Computers in Biology and Medicine reported that AI-assisted PCG could distinguish normal from abnormal heart sounds with over 90% sensitivity in controlled datasets.
Despite these promising findings, real-world diagnostic performance may be lower due to background noise, patient variability, and recording conditions. Consequently, PCG is currently best regarded as a screening or triage tool rather than a definitive diagnostic modality.
Phonocardiography versus Echocardiography:
Although PCG provides objective acoustic analysis of heart
sounds, it cannot directly visualize cardiac anatomy. In contrast,
echocardiography allows detailed assessment of:• valve morphology
• chamber dimensions
• ventricular function
• blood flow patterns
Because of these capabilities, echocardiography remains the gold-standard imaging modality. However, PCG offers several complementary advantages:
Advantages of PCG:
• Non-invasive and inexpensive• Portable and easy to perform
• Suitable for mass screening
• Allows continuous monitoring
• Enables digital storage and telemedicine applications
Advantages of Echocardiography:
• Direct visualization of cardiac structures• Quantitative hemodynamic assessment
• Precise measurement of valve gradients and regurgitation severity
In practical clinical workflows, PCG may be particularly useful for:
• Primary care screening for heart murmurs
• Rural or resource-limited settings where echocardiography is unavailable
• Telemedicine-based cardiac evaluation
• Medical education and auscultation training In such contexts, abnormal PCG findings can serve as a trigger for referral for definitive imaging with echocardiography.
Clinical Scenarios Where PCG Adds Greatest Value:
Based on current evidence, phonocardiography may be
particularly useful in the following settings:
Primary Care Screening
PCG can assist general practitioners in identifying patients who
require referral for echocardiography.
Pediatric Cardiology Screening
Digital PCG systems may help distinguish innocent murmurs from pathological murmurs in children.
Telemedicine and Remote Monitoring
Smartphone-connected digital stethoscopes allow transmission of heart sound recordings for remote expert interpretation.
Role in Medical Education
Declining exposure to classical cardiac auscultation has been reported among medical trainees. Phonocardiography provides a valuable educational tool by allowing learners to visualize heart sounds and correlate them with clinical findings.
Recorded phonocardiograms can be used in teaching sessions to demonstrate characteristic murmurs and improve auscultatory skills. Real-World Limitations
Despite promising research results, several practical challenges remain:
• Dataset bias: Many models are trained on limited or curated datasets.
• Environmental noise: Clinical environments may reduce signal quality.
• Device variability: Different digital stethoscopes produce different signal characteristics.
• Regulatory approval: AI-based diagnostic tools require extensive validation before clinical deployment.
Therefore, AI-assisted PCG systems should currently be considered clinical decision-support tools rather than standalone diagnostic systems.
Pediatric Cardiology Screening
Digital PCG systems may help distinguish innocent murmurs from pathological murmurs in children.
Telemedicine and Remote Monitoring
Smartphone-connected digital stethoscopes allow transmission of heart sound recordings for remote expert interpretation.
Role in Medical Education
Declining exposure to classical cardiac auscultation has been reported among medical trainees. Phonocardiography provides a valuable educational tool by allowing learners to visualize heart sounds and correlate them with clinical findings.
Recorded phonocardiograms can be used in teaching sessions to demonstrate characteristic murmurs and improve auscultatory skills. Real-World Limitations
Despite promising research results, several practical challenges remain:
• Dataset bias: Many models are trained on limited or curated datasets.
• Environmental noise: Clinical environments may reduce signal quality.
• Device variability: Different digital stethoscopes produce different signal characteristics.
• Regulatory approval: AI-based diagnostic tools require extensive validation before clinical deployment.
Therefore, AI-assisted PCG systems should currently be considered clinical decision-support tools rather than standalone diagnostic systems.
Future Directions:
The future of phonocardiography lies in the integration of digital
stethoscopes, wearable sensors, and artificial intelligence. Portable
PCG devices linked to smartphone applications may enable remote
cardiac screening and telemedicine-based diagnosis. With increasing
emphasis on cost-effective healthcare, PCG has the potential to play a
major role in cardiovascular screening programs worldwide.
Conclusion
Phonocardiography represents an objective extension of
traditional cardiac auscultation. Advances in digital technology and
artificial intelligence have renewed interest in this classical diagnostic
method. For clinicians, PCG offers a valuable tool for documenting
heart sounds, improving murmur detection, and enhancing medical
education. While it cannot replace advanced imaging modalities,
phonocardiography may serve as an important adjunct for early
detection and screening of cardiovascular disease.
References
Citation
Das S. Phonocardiography: Revival of Cardiac Auscultation in the Digital Era: A Clinician-Oriented Review. J Cardiobiol. 2026;10(1): 1.