
Journal of Cardiobiology
Download PDF
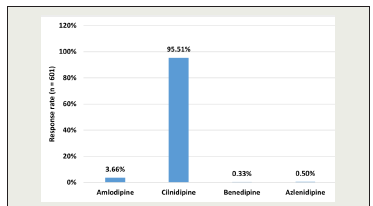 Figure 1:Distribution of responses on the most preferred CCB in patients
with hypertension and DKD
Figure 1:Distribution of responses on the most preferred CCB in patients
with hypertension and DKD
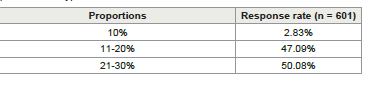 Table 1: Distribution of responses on the use of cilnidipine as first-line therapy in
patients with hypertension and DKD
Table 1: Distribution of responses on the use of cilnidipine as first-line therapy in
patients with hypertension and DKD
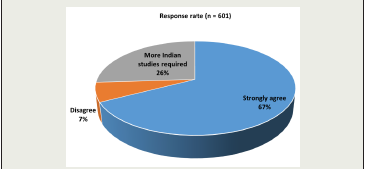 Figure 2:Distribution of responses on the clinicians’ opinions on the
RSSDI guideline recommendation of cilnidipine with ARBs for managing
hypertension in diabetic patients
Figure 2:Distribution of responses on the clinicians’ opinions on the
RSSDI guideline recommendation of cilnidipine with ARBs for managing
hypertension in diabetic patients
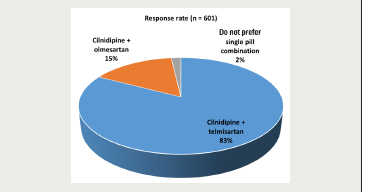 Figure 3:Distribution of responses on the preferred ARB combined with
cilnidipine in diabetic hypertensive patients
Figure 3:Distribution of responses on the preferred ARB combined with
cilnidipine in diabetic hypertensive patients
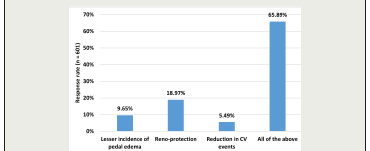 Figure 4:Distribution of responses on the clinical outcomes observed with
cilnidipine beyond BP control
Figure 4:Distribution of responses on the clinical outcomes observed with
cilnidipine beyond BP control
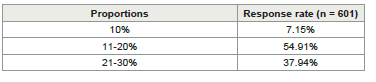 Table 2:Distribution of responses on the proportion of patients on the single-pill
combination of cilnidipine and telmisartan
Table 2:Distribution of responses on the proportion of patients on the single-pill
combination of cilnidipine and telmisartan
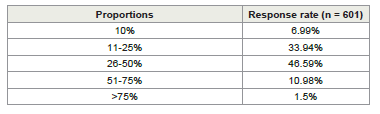 Table 3:Distribution of responses on the clinicians’ experience with cilnidipine in
reducing microalbuminuria among patients with DKD
Table 3:Distribution of responses on the clinicians’ experience with cilnidipine in
reducing microalbuminuria among patients with DKD
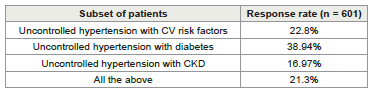 Table 4:Distribution of responses on the subset of patients who most commonly
use telmisartan with cilnidipine single pill combination
Table 4:Distribution of responses on the subset of patients who most commonly
use telmisartan with cilnidipine single pill combination
Research Article
Expert Perspectives on the use of Cilnidipine in Hypertensive Patients with Diabetic Kidney Disease in Indian Settings
Manjula S and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Address for Correspondence:Manjula S, Department of Medical Services, Micro Labs Limited,
Bangalore, Karnataka, India Email Id: drmanjulas@gmail.com
Submission: 20 May, 2025
Accepted: 11 July, 2025
Published: 15 July, 2025
Copyright: ©2025 Manjula S, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Keywords:Cilnidipine; Telmisartan; Hypertension; Diabetic Kidney Disease
Abstract
Objective:To assess clinicians’ preferences and perceptions
regarding the use of cilnidipine, both as monotherapy and in
combination with telmisartan, for managing hypertension in patients
with diabetic kidney disease (DKD) in Indian settings.
Methodology:The cross-sectional study was conducted using a structured 23-item, multiple-response questionnaire designed to capture the perspectives of clinicians involved in the management of hypertension in patients with DKD. The questionnaire focused on current prescribing practices, clinical observations, treatment preferences, and experiences related tocilnidipine both as mono and combination therapy. Data were analyzed using descriptive statistics, and categorical variables were summarized as percentages to highlight prevailing trends and patterns in clinical practice.
Results:The study was conducted among 601 clinicians and revealed that approximately 96% preferred cilnidipine as the calcium channel blocker of choice for patients with hypertension and DKD. Approximately half (50.08%) reported using cilnidipine as a first-line therapy in 21% to 30% of such patients, while 47% used it in 11% to 20% of cases. Most respondents (67.39%) agreed with the RSSDI guideline recommending cilnidipine in combination with angiotensin receptor blockers (ARBs) for enhanced cardiovascular and renal protection. Specifically, 83% favored telmisartan as the ARB of choice in this combination, and 55% reported that 11% to 20% of their patients were on a single-pill cilnidipine-telmisartan regimen. About 66% noted benefits of cilnidipine beyond blood pressure control, including reduced pedal edema, renal protection, and fewer cardiovascular events. Additionally, 47% observed a reduction in microalbuminuria in 26% to 50% of their patients. Around 39% commonly prescribed the cilnidipine-telmisartan single-pill combination for patients with uncontrolled hypertension and diabetes.
Conclusion:Cilnidipine, alone or combined with telmisartan, is widely preferred by Indian clinicians for managing hypertension in patients with DKD, due to its additional benefits beyond BP control, including reno-protection and CV risk reduction.
Methodology:The cross-sectional study was conducted using a structured 23-item, multiple-response questionnaire designed to capture the perspectives of clinicians involved in the management of hypertension in patients with DKD. The questionnaire focused on current prescribing practices, clinical observations, treatment preferences, and experiences related tocilnidipine both as mono and combination therapy. Data were analyzed using descriptive statistics, and categorical variables were summarized as percentages to highlight prevailing trends and patterns in clinical practice.
Results:The study was conducted among 601 clinicians and revealed that approximately 96% preferred cilnidipine as the calcium channel blocker of choice for patients with hypertension and DKD. Approximately half (50.08%) reported using cilnidipine as a first-line therapy in 21% to 30% of such patients, while 47% used it in 11% to 20% of cases. Most respondents (67.39%) agreed with the RSSDI guideline recommending cilnidipine in combination with angiotensin receptor blockers (ARBs) for enhanced cardiovascular and renal protection. Specifically, 83% favored telmisartan as the ARB of choice in this combination, and 55% reported that 11% to 20% of their patients were on a single-pill cilnidipine-telmisartan regimen. About 66% noted benefits of cilnidipine beyond blood pressure control, including reduced pedal edema, renal protection, and fewer cardiovascular events. Additionally, 47% observed a reduction in microalbuminuria in 26% to 50% of their patients. Around 39% commonly prescribed the cilnidipine-telmisartan single-pill combination for patients with uncontrolled hypertension and diabetes.
Conclusion:Cilnidipine, alone or combined with telmisartan, is widely preferred by Indian clinicians for managing hypertension in patients with DKD, due to its additional benefits beyond BP control, including reno-protection and CV risk reduction.
Introduction
With the increasing worldwide prevalence of type 2 diabetes
mellitus (T2DM), diabetic kidney disease (DKD) has emerged as a
significant contributor to the global disease burden.[1] DKD ,or
diabetic nephropathy, is the most common cause of chronic kidney
disease(CKD) in those with diabetes and is the leading attributable
cause for incident end-stage renal disease (ESRD).[2] The burden
of hypertension is even greater in those with comorbid CKD,
with prevalence risingparallel with disease severity. A nationally
representative U.S. survey estimated hypertension in 23.3% of
individuals without CKD, compared to 35.8% in stage 1, 48.1%
in stage 2, 59.9% in stage 3, and 84.1% in stages 4-5.[3] Globally,
hypertension affects approximately 70% to 90% of patients with
diabetic nephropathy, with prevalence increasing parallelly with
CKD severity. [3] The Indian Chronic Kidney Disease (ICKD) study
found that 87% of CKD patients in the country are hypertensive, and
37% have diabetes.[4]
Effective blood pressure (BP) management in this subset of
patients presents a therapeutic challenge, requiring agents that
not only ensure optimal BP control but also provide cardio-renal
protection. Among the available antihypertensive therapies, calcium
channel blockers(CCBs) have garnered considerable attention due to
their efficacy and safety profile. [5] Cilnidipine, a fourth-generation
dihydropyridine CCB with dual L/N-type CCB activity, has gained
attention for its potential reno-protective and cardio-protective
benefits beyond BP reduction.[6] This unique pharmacologic profile
is proposed to offer advantages beyond BP control, including a
reduction in sympathetic overactivity, a lesser incidence of pedal
edema, improved renal outcomes, and favorable metabolic effects
such as improved insulin sensitivity.[7,8]
As per the Joint National Committee (JNC) 8 recommendations,
CCB is recommended as initial therapy in patients with hypertension,
including those with diabetes.[9] Cilnidipine is used in the
management of hypertension and comorbid conditions either as a
monotherapy or as a combination therapy with angiotensin receptor
blockers (ARBs). [10,11] This is achieved through a reduction in
urinary albumin excretion and an increase in the ratio of Ang (1–
7) to Ang II in plasma.[12] The Research Society for the Study of
Diabetes in India (RSSDI) has recommended the use of cilnidipine
in combination with ARBs such as telmisartan for enhanced
cardiovascular and renal protection.[13]This study is intended to
gather expert opinion on the use of cilnidipine and its combination
with telmisartan for managing hypertension with DKD in Indian
settings.
Methodology
We carried out a cross-sectional study among experts managing
hypertensive patients with DKD in Indian clinical settings from June
2024 to December 2024. Clinicians from diverse specialties, including
general physicians, diabetologists, and cardiologists, were invited to
participate. The study was conducted after receiving approval from
Bangalore Ethics, an Independent Ethics Committee, which was
recognized by the Indian Regulatory Authority, the Drug Controller
General of India (ECR/355/Indt/KA/2022).
An invitation was sent to leading clinicians in managing
hypertensive patients with DKD in the month of March 2024 for
participation in this Indian survey. About 601 clinicians from major
cities of all Indian states, representing the geographical distribution,
shared their willingness to participate and provide necessary data.
The questionnaire booklet titled NEPCAR (Nephro Cardio protective
calcium channel blocker) was sent to clinicians who were interested
in participating in this study. The NEPCAR study questionnaire
comprised 23 questions focusing on current practices, clinical
observations, and specialist experiences in managing hypertension
in patients with DKD, with particular emphasis on the routine
use of cilnidipine, both as monotherapy and in combination with
telmisartan. Clinicians had the option to skip any questions they
preferred not to answer. They were instructed to complete the
questionnaire independently, without consulting their colleagues.
Written informed consent was obtained from all participants before
the study commenced.
Statistical analysis:
The data collected were analyzed using descriptive statistics.
Categorical variables were presented as percentages to provide a clear
insight into their distribution. The frequency of occurrence and the
corresponding percentage were used to represent the distribution
of each variable. To visualize the distribution of the categorical
variables, graphs and pie charts were created using Microsoft Excel
2013 (version 16.0.13901.20400).
Results
The study included 601 experts, and approximately 40% of them
reported that 21% to 30% of patients with hypertension presenting to
the routine settings have both comorbid diabetes and CKD. Around
45% of clinicians stated that 26% to 50% of patients with DKD and
hypertension experience BP variability, while 44% reported that
11% to 25% of such patients suffer from BP variability. A significant
majority (95.51%) of respondents identified cilnidipine as the most
preferred CCB for managing hypertension in patients with DKD
[Figure 1].
Half of the experts (50.08%) reported using cilnidipine as a firstline
therapy in 21% to 30% of patients with hypertension and DKD,
while 47% stated they prescribe it in 11% to 20% of such patients
[Table 1]. About 31% of clinicians observed that cilnidipine improves
renal parameters, including urinary protein-to-creatinine ratio
(UPCR), urinary protein excretion (UPE), and estimated glomerular
filtration rate (eGFR)in some patients.
About 49% of the clinicians stated that they were unsure whether
cilnidipine improves creatinine levels compared to amlodipine in
patients. More than half (58.07%) of the participants reported that
approximately 11% to 20% of patients with hypertension have elevated
creatinine levels. According to 45% of the experts, hypertensive
patients aged 46 to 60 years commonly exhibit high creatinine levels.
A majority of clinicians (67.39%) agreed that, according to
the RSSDI guidelines for managing hypertension in patients with
diabetes mellitus, cilnidipine is recommended in combination with
angiotensin receptor blockers (ARBs) to enhance cardiovascular
and renal protection in diabetic hypertensive patients [Figure 2]. As
reported by 43% of the respondents, about 10% to 20% of patients
with hypertension achieve control with monotherapy.
The majority of clinicians (82.7%) reported preferring the
combination of cilnidipine with telmisartan as the specific ARB for use
in diabetic hypertensive patients [Figure 3]. More than half (54.91%)
of the experts stated that 11% to 20% of their patients are currently
on the single-pill combination of cilnidipine and telmisartan
[Table 2]. Nearly half of the clinicians (47.75%) reported that 21% to 30% of
their patients, who are currently receiving a combination of a renin–
angiotensin–aldosterone system (RAAS) blocker and a diuretic,
could be shifted to a cilnidipine and telmisartan combination.
About 66% of the participants reported a lower incidence of pedal
edema, renal protection, and a reduction in cardiovascular (CV)
events as clinical outcomes observed in patients receiving cilnidipine,
beyond its BP-lowering effects [Figure 4]. Approximately 48% of the
participants stated that 11% to 30% of hypertensive patients tested
positive for proteinuria.
Around 47% of clinicians reported that cilnidipine reduced
microalbuminuria in 26% to 50% of their patients [Table 3].
Approximately 66% of participants identified reduced pedal edema
as a key advantage of cilnidipine. As reported by 64% of experts,
the combination of telmisartan with cilnidipine is preferred for BP
control and cardiorenal protection in middle-aged patients.
Around 39% of participants reported that they commonly
prescribe a single-pill combination of telmisartan with cilnidipine
for patients with uncontrolled hypertension and diabetes [Table 4].
Almost half of the clinicians (49.75%) were unsure about considering
cilnidipine as their preferred antihypertensive agent in the
management of hypertension. According to approximately 45% of
clinicians, low awareness about hypertension may be a contributing
factor to CV disease-related deaths in patients aged 40 to 59 years.
Approximately 44% of clinicians opined that cilnidipine also
improves insulin resistance in obese hypertensive patients, while 42%
indicated that improvement in insulin resistance is observed only in
a few cases. Around 47% of clinicians reported conducting monthly
follow-ups for patients with uncontrolled hypertension and DKD.
Discussion
In the present study, the majority (95.51%) of the clinicians
preferred cilnidipine as the CCB of choice for managing hypertension
in patients with DKD, reflecting growing clinical confidence in its
reno-protective properties. In line with this, Mehta et al. stated that
cilnidipine is the most common CCB used antihypertensive agent
due to its effectiveness in reducing BP, along with its good tolerability
and evidence of reducing hypertension, related cardiovascular and
renal diseases.[12] Srivathsan et al. concluded that cilnidipine is
more effective in reducing proteinuria or preventing its progression,
while demonstrating comparable effects on serum creatinine and
estimated glomerular filtration rate (eGFR) in hypertensive patients.
[14] Similarly, Chakraborty et al. recommended cilnidipine as a novel
first-line CCB for managing hypertension, either as monotherapy or
in combination.[10]
The present study also revealed that clinicians frequently
prescribed cilnidipine as a first-line treatment in patients with
hypertension and DKD, indicating its growing acceptance in routine
clinical practice. Supporting this, the J-CIRCLE study evaluated 70
hypertensive patients with chronic kidney disease who continued
to have albuminuria despite amlodipine therapy. After switching to
cilnidipine for three months, patients showed a significant reduction
in the urinary albumin-to-creatinine ratio, despite no significant
change in blood pressure. Notably, cilnidipine also reduced uric acid
levels in patients with elevated baseline values, highlighting additional
metabolic benefits beyond its antihypertensive effects.[15]
The current study findings align with the recommendations of
the RSSDI, which suggests that cilnidipine, as a novel CCB, should
be used in combination with ARBs for enhanced cardiovascular and
renal protection in diabetic hypertensive patients.[13] Supporting
this, a randomized controlled trial by Katayama et al. (2006) involving
87 patients with type 2 diabetes and albuminuria found that the
combination of cilnidipine and valsartan led to a significantly greater
reduction in the urinary albumin-to-creatinine ratio compared to
valsartan alone (−44% vs. −9%, P = 0.014).[16] The HOPE-Combi
survey carried out by Kario et al. (2020) demonstrated that a single-pill
combination of cilnidipine and valsartan effectively reduced morning
home systolic BP and pulse pressure in patients with uncontrolled
hypertension and sympathetic hyperactivity.[17]
The majority of the current study clinicians indicated a preference
for combining cilnidipine with telmisartan as the ARB of choice in
managing diabetic hypertensive patients. Additionally, more than
half of the experts reported that 11% to 20% of their patients were
receiving the single-pill combination of cilnidipine and telmisartan.
Similarly, in a knowledge, attitude, and practice survey conducted
by Shete et al., the cilnidipine and telmisartan combination was
reported to benefit patients with uncontrolled hypertension (46%),
diabetes (43%), and chronic kidney disease (41%), making it a
preferred therapeutic option.[18] Jo et al. also suggested that the
combination of cilnidipine and telmisartan serves as an effective
therapeutic strategy for managing hypertension and its associated
complications.[19] Furthermore, a prospective randomized study
conducted at three tertiary hospitals in India concluded that this
combination significantly reduced blood pressure and improved
central hemodynamic parameters, such as the aortic augmentation
index, in patients with untreated or uncontrolled hypertension [20].
Majority of the survey respondents cited reduced incidence of
pedal edema, reno-protection and reduction in CV events askey
clinical outcomes observed in patients receiving cilnidipine, beyond
its BP lowering effects. The study also indicated that cilnidipine
is effective in reducing microalbuminuria. Kumari et al. similarly
reported that cilnidipine demonstrates superior renoprotective
effects, as evidenced by a significant reduction in proteinuria among
hypertensive patients.[21] Ramya et al. noted satisfactory BP control
with negligible side effects and a lower incidence of pedal edema in
patients treated with cilnidipine.[22] Chandra and Ramesh found
that cilnidipine exhibits renoprotective, cardioprotective, and
neuroprotective effects.[6] Pavan Malleshappa also reported that
cilnidipine is safe and effective in reducing low-grade albuminuria in
hypertensive CKD patients.[23] Additionally, Singh et al. concluded
that cilnidipine has an additive effect in reducing microalbuminuria.
[24]
The current study reported that clinicians commonly prescribe
the single-pill combination of telmisartan and cilnidipine for patients
with uncontrolled hypertension and diabetes. Sawant et al. concluded
that once daily cilnidipine and telmisartan is effective and well
tolerated in the treatment of newly diagnosed stage I hypertension
[25]. A cross-sectional survey involving 533 clinicians in India
revealed that 76% recommended the cilnidipine and telmisartan
combination for diabetic hypertensive patients, citing its efficacy in
blood pressure reduction, cardioprotective effects, and the added
benefit of attenuating high blood glucose levels.[8]
The study provides valuable insights into clinicians’ preferences
regarding the use of cilnidipine for managing hypertension in
patients with DKD in the Indian context. Despite its strengths, such
as a large and diverse sample of clinicians and the use of a structured
questionnaire, several limitations should be acknowledged. The study
captures expert opinion rather than objective clinical outcomes,
which introduces potential bias due to individual differences in
clinical judgment, experience, and prescribing patterns. In addition,
the cross-sectional design limits the ability to assess trends over time,
treatment effectiveness, or patient outcomes. Since the findings are
based on clinicians’ perceptions, they do not reflect actual patient data,
such as changes in kidney function or cardiovascular events, which
may reduce the broader applicability of the results. Furthermore,
the study may not fully capture evolving treatment practices or the
influence of the latest clinical evidence. Future studies should include
prospective or observational research involving direct patient data
to validate these observations and support more informed treatment
strategies for this population.
Conclusion
The study highlights that cilnidipine is widely preferred by Indian
clinicians for the management of hypertension in patients with DKD,
both as monotherapy and in combination with telmisartan. The
preference is supported by its perceived benefits beyond BP control,
including reduced incidence of pedal edema, reno-protective effects,
and CV risk reduction. The strong alignment with RSSDI guideline
recommendations and the frequent use of single-pill combinations
underscore the growing clinical confidence in cilnidipine, particularly
when paired with telmisartan, as a practical and effective therapeutic
option in this high-risk population.
Acknowledgement
We would like to thank all the clinicians who were actively
participating in this study.
Disclosure of compliance with ethical principles:
The study was conducted after receiving approval from Bangalore
Ethics, an Independent Ethics Committee, which was recognized by
the Indian Regulatory Authority, Drug Controller General of India.
References
Citation
Manjula S, Kumar MK. Expert Perspectives on the use of Cilnidipine in Hypertensive Patients with Diabetic Kidney Disease in Indian Settings. J Cardiobiol. 2025;9(1): 1.