
Case Report
*Address for Correspondence: Shaun Cardozo, M.D., Division of Cardiology, Harper University Hospital 8 Brush, 3990 John R, Detroit, MI 48201, USA, Tel: 313-745- 2620; Fax: 313-745 8643; E-mail: scardozo@med.wayne.edu
Citation: Kaur R, Jacob S, Cardozo S. Lithium Toxicity and Level Dependent Sinoatrial Exit Block. J Cardiobiol. 2013;1(1): 1.
Copyright © 2013 Kaur R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cardiobiology | ISSN: 2332-3671 | Volume: 1, Issue: 1
Submission: 10 September 2013 | Accepted: 19 September 2013 | Published: 24 September 2013
Reviewed & Approved by: Dr. Krasniqi Nazmi, Division of Cardiology, University Hospital of Zurich, Switzerland
74 year old nursing home patient with known history of schizoaffective disorder, hypertension and dementia was brought to the emergency room due to altered mental status and disorientation. Vitals on admission were stable and the initial 12-lead EKG showed an irregular rhythm with a 3 second pause and a narrow QRS complex with no obvious ST-segment elevation or depression. Later the patient had several long pauses (6-7 seconds) and became hypotensive. Sinoatrial (SA) exit block was noted on the monitor (Figure 1). Pertinent labs on admission showed a sodium level of 150 mmol/L, blood urea nitrogen of 26 mg/dL, creatinine of 1.6 mg/dl, leukocytosis (25.6 x 109/L) and the lithium levels of 2.5 mEq/L (normal: 0.7-1.5 mEq/L).
In addition to initiating work up of sepsis, given the sinus pause, transcutaneous pacemaker pads were placed with good ventricular capture. The patient with a presumptive diagnosis of lithium toxicity was admitted to ICU for cardiac monitoring, intravenous hydration and serial lithium levels. She responded well to intravenous hydration and lithium levels started trending down to 0.8 mEq/L on day 3. The cardiac conduction abnormality improved over a period of 24 hours and the transcutaneous pacemaker was discontinued and the patient was transferred to the floor in stable condition.
Lithium Toxicity and Level Dependent Sinoatrial Exit Block
Ramanjit Kaur1, Sony Jacob2 and Shaun Cardozo2*
- 1Department of Internal Medicine, Harper University Hospital, Wayne State University, Detroit, Michigan, USA
- 2Division of Cardiology, Harper University Hospital, Wayne State University, Detroit, Michigan, USA
*Address for Correspondence: Shaun Cardozo, M.D., Division of Cardiology, Harper University Hospital 8 Brush, 3990 John R, Detroit, MI 48201, USA, Tel: 313-745- 2620; Fax: 313-745 8643; E-mail: scardozo@med.wayne.edu
Citation: Kaur R, Jacob S, Cardozo S. Lithium Toxicity and Level Dependent Sinoatrial Exit Block. J Cardiobiol. 2013;1(1): 1.
Copyright © 2013 Kaur R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cardiobiology | ISSN: 2332-3671 | Volume: 1, Issue: 1
Submission: 10 September 2013 | Accepted: 19 September 2013 | Published: 24 September 2013
Reviewed & Approved by: Dr. Krasniqi Nazmi, Division of Cardiology, University Hospital of Zurich, Switzerland
Abstract
Background: Lithium toxicity has been associated with variable changes on Electrocardiogram (ECG) but several long pauses secondary to Sinoatrial (SA) exit block have not been formally reported.Conclusion: Our case highlights that in chronic lithium patients presenting with altered mental status and conduction problems, an emergency physician should have a high index of suspicion for lithium toxicity and appropriate therapy to be initiated expeditiously. Further experiments on human and animal models involving molecular pharmacology and electrophysiology are necessary to understand the sinus node/perisinus tissue electrophysiological behavior caused by Lithium.
74 year old nursing home patient with known history of schizoaffective disorder, hypertension and dementia was brought to the emergency room due to altered mental status and disorientation. Vitals on admission were stable and the initial 12-lead EKG showed an irregular rhythm with a 3 second pause and a narrow QRS complex with no obvious ST-segment elevation or depression. Later the patient had several long pauses (6-7 seconds) and became hypotensive. Sinoatrial (SA) exit block was noted on the monitor (Figure 1). Pertinent labs on admission showed a sodium level of 150 mmol/L, blood urea nitrogen of 26 mg/dL, creatinine of 1.6 mg/dl, leukocytosis (25.6 x 109/L) and the lithium levels of 2.5 mEq/L (normal: 0.7-1.5 mEq/L).
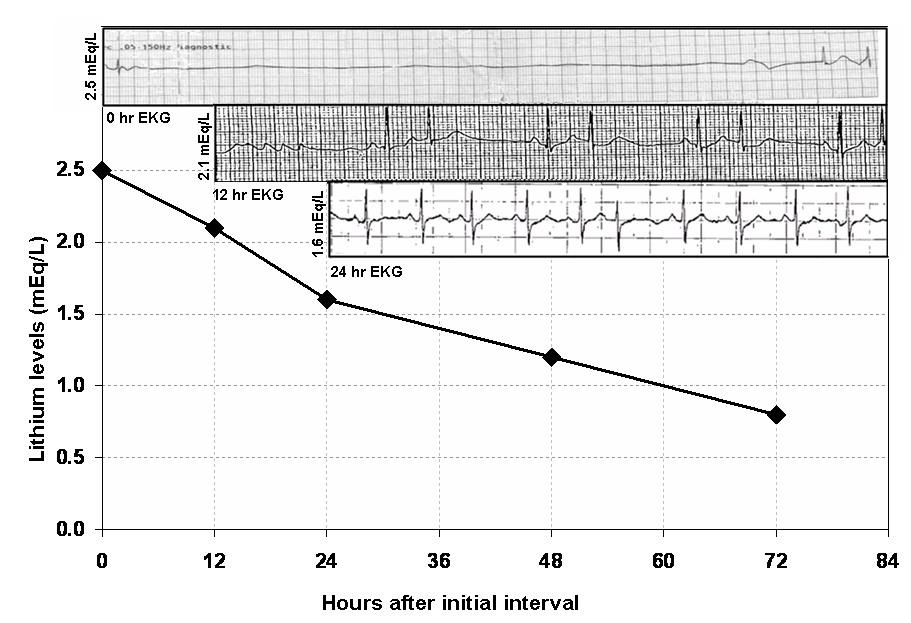
Figure 1: Lithium Level Dependent Sinoatrial Exit Block: At 0- hour, when the lithium level was 2.5 mEq/L, there was 3rd degree sinoatrial exit block or sinus standstill. At around 2.1 mEq/L, it showed second degree sinoatrial block. The sinoatrial conduction block improved completely resuming normal sinus rhythm at 24 hrs when the lithium level was around 1.6 mEq/L.
Lithium is known to be associated with a variety of cardiac conduction abnormalities. We report EKG findings with lithium dose dependent spectrum of Sinoatrial exit block. The EKG on admission with lithium level of 2.5 revealed 3rd degree sinoatrial exit block demonstrating complete absence of P wave and only AV-junctional escape rhythm which gradually transformed in 12 hrs with IV hydration to 2nd degree sinoatrial exit block. The sinoatrial conduction block improved completely resuming normal sinus rhythm at 24 hrs when the lithium level was 1.6 mEq/L.
Lithium salts are widely used in treatment and prophylaxis as mood stabilizers like mania, bipolar affective disorder, recurrent depression and aggressive or self- mutilating behavior. Lithium is fully absorbed after oral intake approximately in 8 hrs with peak level occurs at 2 to 4 hrs [1]. The therapeutic range varies from 0.7 - 1.5 mEq/L. The plasma elimination half life of a single dose of lithium is between 12 - 27 hrs [2,3].
Animal experiments indicate that lithium depresses the intracellular potassium concentration as well as replaces intracellular calcium which results in various electrophysiological changes including a decrease of the depolarization rate and reduced electrical impulse propagation [4]. It also has been suggested regarding lithium decreasing the sensitivity of sinus node to sympathetic stimulation [5]. Further experiments on human and animal models involving molecular pharmacology and electrophysiology are necessary to understand the sinus node/perisinus tissue electrophysiological behavior caused by Lithium.
References
- Baldessarini RJ (1990) Drugs and treatment of psychiatric disorders. In: Gilman. A, G., Goodman, L. S., Rall, T, W., Murad, F. (eds.) Goodman and Gilman's Pharmacological basis of therapeutics (8th edn.) pp: 383-435. New York: Pergamon Press.
- Amdisen A (1975) Monitoring of lithium treatment through determination of lithium concentration. Dan Med Bull 22: 277-291.
- Thornhill DP (1978) Pharmacokinetics of ordinary and sustained-release lithium carbonate in manic patients after acute dosage. Eur J Clin Pharmacol 14: 267-271.
- El-Mallakh RS (1990) The ionic mechanism of lithium action. Lithium 1: 87-92.
- Fann WE, Davis JM, Janowsky DS, Cavanaugh JH, Kaufmann JS, et.al. (1972) Effects of Lithium on adrenergic function in man. Clin Pharmacol Ther 13: 71-77.