
Journal of Addiction & Prevention
Download PDF
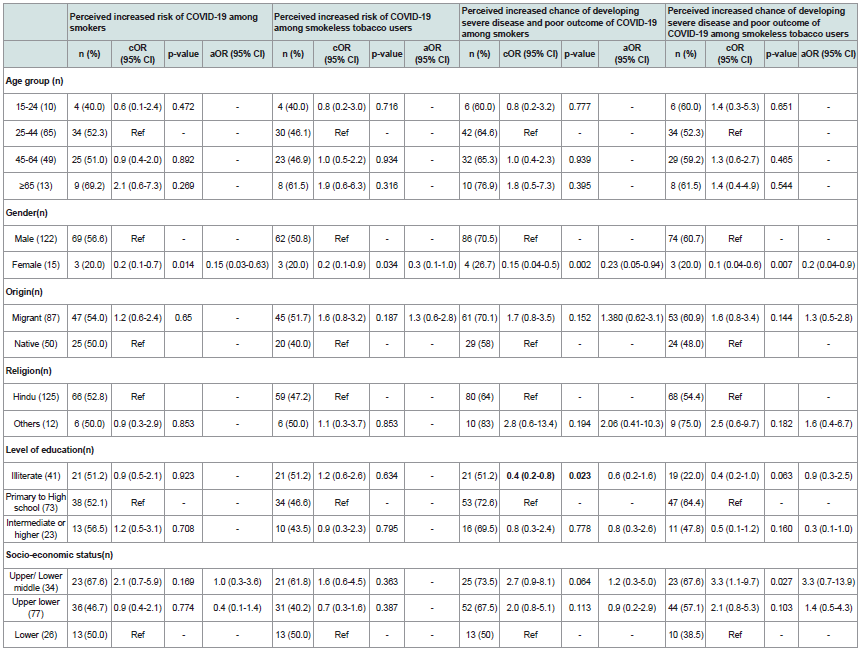 Table 1: Perceptions about COVID-19 infection among tobacco users
Table 1: Perceptions about COVID-19 infection among tobacco users
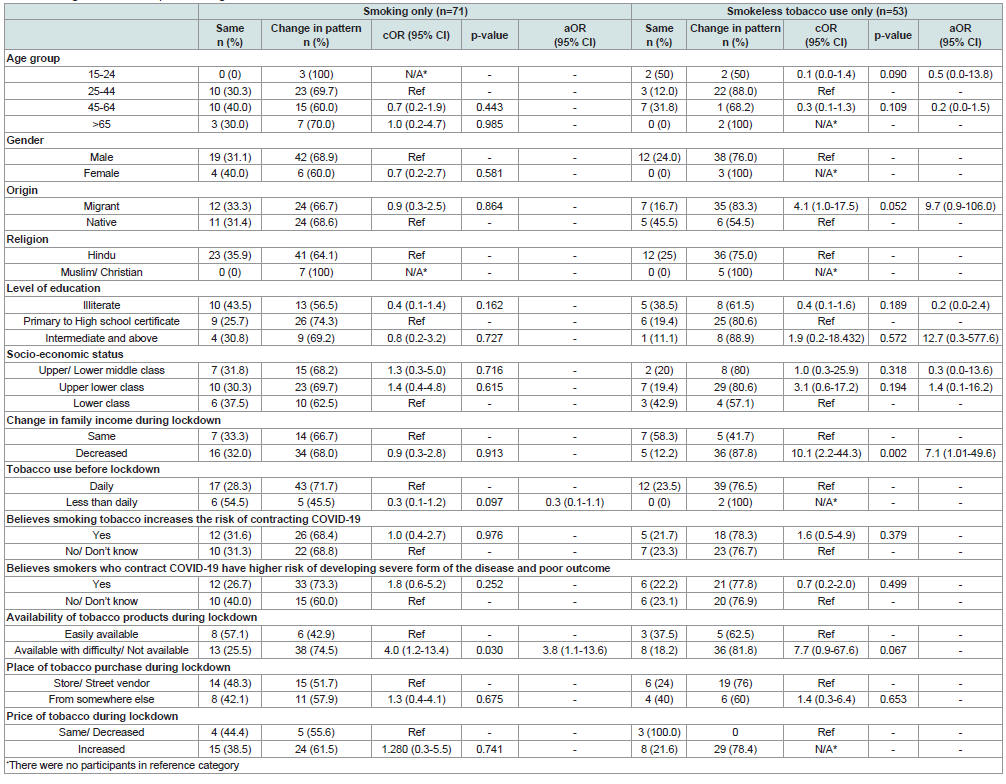 Table 2: Change in tobacco use pattern during lockdown and associated factors.
Table 2: Change in tobacco use pattern during lockdown and associated factors.
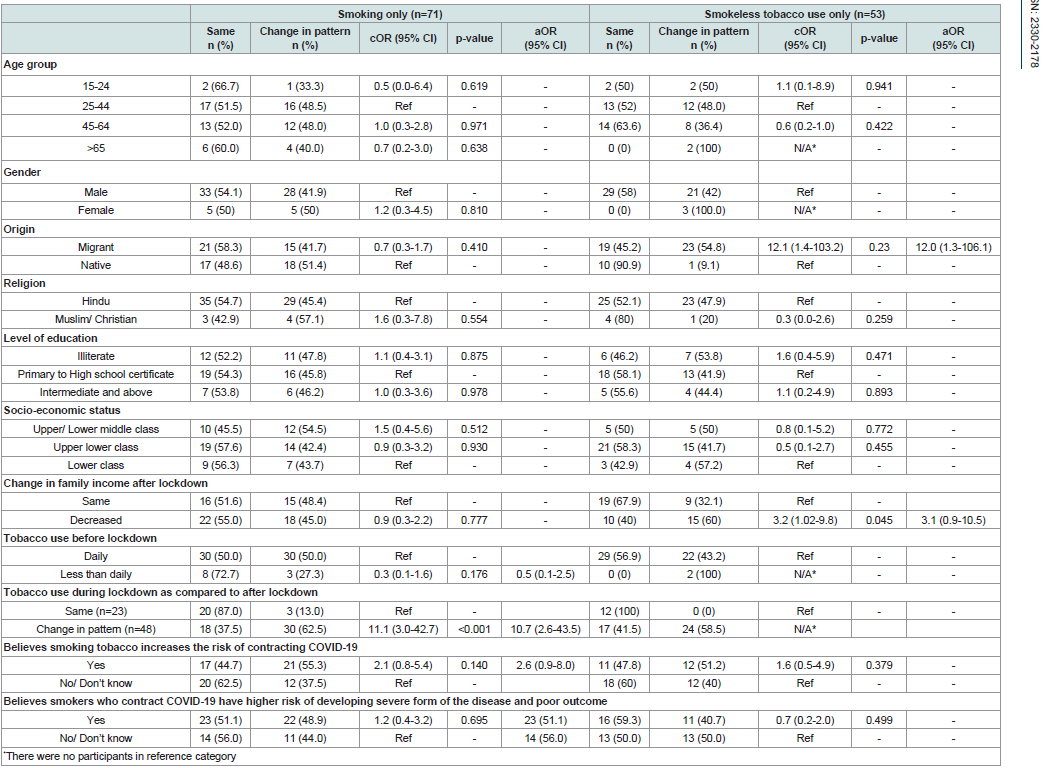 Table 3: Change in tobacco use pattern after lockdown and associated factors.
Table 3: Change in tobacco use pattern after lockdown and associated factors.
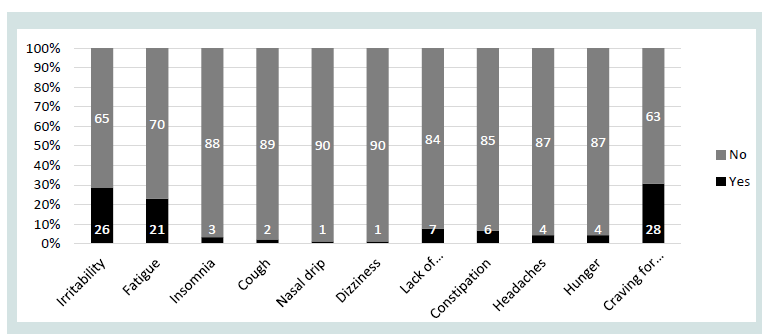 Figure 1: Experiencing of different withdrawal symptoms during lockdown on
decreasing or stopping tobacco use (n=91).
Figure 1: Experiencing of different withdrawal symptoms during lockdown on
decreasing or stopping tobacco use (n=91).
Research Article
Change in Patterns of Tobacco Use during Lockdown due to COVID-19
Yukti B1* , Kishore J1 and Jagdish K2
1Department of Community Medicine,Vardhman Mahavir Medical
College and Safdarjung Hospital, India
2Tobacco Free Initiative World Health Organization Regional Office
for South-East Asia, India
*Address for Correspondence:
Yukti B, Vardhman Mahavir Medical College and Safdarjung Hospital,
Ansari Nagar, Delhi, India; Tel: 8130998281; Email: dr.yuktibhandari@
gmail.com
Submission: 24 December, 2021;
Accepted: 25 January, 2022;
Published: 29 January, 2022
Copyright: © 2022 Yukti B, et al. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
Introduction:
Tobacco consumption is among the biggest public
health concerns globally, causing disease, disability, premature
deaths with additional economic, social and environmental burden.
The COVID-19 pandemic led to a nationwide lockdown in India which
affected tobacco consumption due to various reasons.
Objectives:
This community-based-cross-sectional study aimed to
assess the change in patterns of tobacco use during and after the
lockdown. It also attempted to assess access to tobacco, withdrawal
symptoms experienced, and perceptions about association of
tobacco use with COVID-19.
Methods:
The study was conducted in Aliganj, an urbanized
village, in South Delhi. 140 adults(aged >15 years) who used tobacco
before the lockdown, residing in Aliganj were included in the study.
Data was analysed using SPSS-21.
Results:
The prevalence of change in pattern of tobacco
use during lockdown was 71.4% (66.7% smokers, 77.4% smokeless
tobacco(SLT) users, 73.3% dual users). Quitting tobacco reported by
27.8% smokers, 30.2% SLT users, 13.3% dual users. A change in pattern
after lockdown reported by 49.3% (45.8% smokers, 45.3% SLT users, 80%
dual users). 46.2% reported experiencing withdrawal symptoms.
Difficult availability of tobacco during lockdown reported
by 60.0% and unavailability by 15.2%. Increased risk of COVID-19
infection among smokers and higher risk of developing severe disease
perceived by 51.4% and 64.3%, respectively.
Conclusion:
Clear impact of lockdown on tobacco use is
indicated by the difference between change in tobacco use pattern
during and after lockdown. Lockdown restrictions led to decreased
income, increased prices and decreased availability of tobacco,
which were major reasons for changed pattern during lockdown.
Lifting of restrictions (post lockdown period) resulting in return to
regular pricing, availability of tobacco products and lack of support
for those who experienced withdrawal symptoms, caused return to old
patterns of usage after lockdown. The factors identified in this study, if
translated to policy change, might be effective in reducing tobacco
usage during the pandemic and beyond.
Introduction
Tobacco consumption is among the most significant public
health concerns globally. Tobacco is consumed in various formsboth
smoked and smokeless. Smoked forms of tobacco include
cigarettes, bidi, hukkah (water-pipes), etc. Smokeless forms of
tobacco include chewing tobacco, gutkha, khaini, betel quid mixed
with tobacco, zarda, mawa, mishri, gudaku etc. Tobacco use is known
to cause chronic illnesses like lung diseases, cardiovascular diseases,
cancers, and stroke. Tobacco-related deaths and diseases in low- and
middle-income countries contribute to 80% of the global burden [1].
According to the report by the Global Adult Tobacco Survey (GATS)
in India during 2016-2017, about 28.6% adults (>15 years) used
tobacco. GATS also revealed that 17.8% adults in Delhi used tobacco
[2].
Tobacco use is related to poverty as it causes financial stress on low-income families with the diversion of family income used to
meetessential household expenses. The COVID-19 pandemic led to
a nationwide lockdown from 25th March’20 in India. The gradual
relaxation of lockdown began from 1st June’20 with continued
restrictions in containment zones (areas with high prevalence of
COVID-19). During the lockdown, people also experienced financial
hardships due to decreased income.Shops selling and providing nonessential
goods or services including tobacco products were closed.
Contaminated hands and cigarettes/bidis may increase the risk
of contracting COVID-19 while smoking. Hukkah is commonly
used in communal settings, increasing the chances of contracting
COVID-19through sharing of mouth-piece among users. During the
lockdown, most of the population remained indoors, which could
have increased the exposure of second-hand smoke among family
members of smokers. Chewing of tobacco also leads to spitting.
Spitting in public places by a SARS-CoV-2 infected person can increase
the risk of spreading the virus in the community. Several studies have
been conducted about the effect of smoking on covid-19. They have
established an association between tobacco use and increased risk
of contracting covid-19 and a severe form of the disease with poor
outcomes such as the need for ICU care, mechanical ventilation, or
mortality [3,,6,7,8,9]. Few studies have been conducted on the change
in patterns of tobacco use during lockdown [4,5].
This study was planned to assess the alteration in patterns of
tobacco use during lockdown due to COVID-19 amongst adults
residing in a community in New Delhi and to study the factors
associated with alteration in that patterns of tobacco use.
Methods
It is a community-based-cross-sectional study conducted in
Aliganj, an urbanized village in the South District of Delhi. The
total adult population of the area is over 6000 residing in about
1668 households. Migrants contribute a significant percentage of
the population. Lockdown in Delhi started on 25th March’20, and
unlocking was done in phases from 1st June’20 with continued restrictions in identified containment areas. The lockdown restrictions
were gradually relaxed in the village from 1st July’20. Adults (>15
years) who used tobacco before the lockdown and residing in Aliganj
for the past six months were included in the study.
Elias M. Klemperer et al. observed that 58.6% of study participants
changed (increase or decrease) in tobacco consumption patterns
during the lockdown [4].
Taking Zα/2= 1.96 (critical value of the normal distribution at
95% confidence), 15% relative error and adding 10% non-response
rate the sample size was 133 persons. However, a total of 140 were
included in the study.
Consecutive sampling was done in this community survey. The
first house was chosen at random. Every adult fulfilling the inclusion
criteria was included in the study until the sample size was completed.
A pre-tested, semi-structured, interviewer-administered
questionnaire prepared using validated tools after a thorough review
of the available literature was used to collect data. The questionnaire
included socio-demographic details (Modified Kuppuswamy scale
[16,17] for socioeconomic status), perceptions about the association
of tobacco use and COVID-19, access to tobacco products during
lockdown, change in patterns of tobacco use and other substances.
The questionnaire was translated in Hindi with the standard method,
which was the community’s local language.
Data collection was completed in March’21 using the
questionnaire by the first author. Data entry was done simultaneously.
The study’s primary outcome was the change in patterns of tobacco
use during lockdown due to the COVID-19 pandemic. The study’s
secondary outcome was the change in patterns of tobacco use after
lockdown due to COVID-19 pandemic. The factors studied included
socio-demographic factors, perception about covid-19 and tobacco
use, and access to tobacco products during lockdown.
Data were checked for errors and missed values and entered in
Microsoft Excel. Data analysis was done using Statistical Package for
the Social Sciences-Version 21(SPSS-21). Socio-demographic details
and changes in the pattern of tobacco usage of the study population
have been described using frequencies and percentages. The study
population has been divided into sub-groups of smokers, smokeless
tobacco (SLT) users, and dual users (using both smoked and SLT).
Appropriate cross tables and tests of significance have been used to
study associations; p-values <0.05 have been taken as significant, but
an association of variables having a p-value<0.2 were entered into the
model for calculating adjusted odds ratio (aOR).
Results
The age of study participants ranged from 17-86 years. The mean
age of participants was 43.3 (±14.2 years), with 90.3% males. Of the
140 participants, 51.4% used smoked tobacco, 37.8% used SLT, and
10.7% were dual users. The majority of the participants were Hindus
(91.4%). Most of the participants were migrants from outside Delhi
(64.3%). Of the study population, 31.4% were illiterate, 16.4% were
educated beyond secondary school. None of the participants were
classified as upper class as per the Modified Kuppuswamy scale,
revised for 2020. Half of the participants belonged to the upper
lower class. A decrease in total family income during the lockdown compared to before the lockdown was reported by 74.3%, and 52.1%
reported a decreased family income after the lockdown. None of the
study participants reported an increase in total family income either
during or after lockdown. During lockdown, tobacco was easily
available for 16.4% participants, available with difficulty for 60.0%
participants, and not available to 15.7% participants; 7.8% did not
know or refused to answer. Tobacco was purchased from store/street
vendors by 42.1%, 21.4% bought it from someone else, and 30.7%
reported not purchasing it during the lockdown. An increase in prices
of tobacco during lockdown was reported by 60.0%. An increased
risk of contracting COVID-19 among smokers as compared to nonsmokers
was perceived by 51.4%. An increased risk of contracting
COVID-19 among SLT users was perceived by 54.3%. An increased
chance of developing severe disease and poor outcome of COVID-19
among smokers on contracting the infection was believed by 64.3%,
and 55.0% believed that there is an increased chance of developing
severe disease and poor outcome of COVID-19 among SLT users on
contracting the infection.
Table 1 shows, gender was significantly associated with the
perception of increased risk of contracting COVID-19 infection
among tobacco users. About 69% of the males perceived smoking
to be associated with an increased risk of contracting COVID-19
infection, whereas 66% of the females did not have any knowledge
of the same. However, lesser odds of increased risk of COVID-19
among tobacco users were observed among females (OR: 0.1;
95%CI 0.03-0.63). About half (50.8%) of the males perceived SLT
use associated with an increased risk of contracting COVID-19
infection. In contrast, the majority (66.7%) of the females did not
have any knowledge of the same. The majority (70.5%) of the males
perceived an increased chance of developing severe disease and poor
outcome of COVID-19 among smokers on contracting the infection.
Among males, 60.6% perceived an increased chance of developing
severe disease and poor outcome of COVID-19 among SLT users
on contracting the infection. In contrast, the majority (73.3%) of the
females did not have any knowledge of the same. Females had lesser
odds of perceiving the use of SLT as a risk factor for developing severe
COVID-19 infection (aOR 0.2; 95%CI: 0.04-0.9). Of the 72 smokers,
83.3% smoked tobacco daily before the lockdown, and 16.7% smoked
tobacco products but not daily. Of the 53 SLT users, 96.2% used only
SLT daily before the lockdown, and 3.8% used only SLT products
but not daily. Among 15 dual users, 66.7% of participants used both
smoked and SLT products daily, 13.3% of participants used smoked
tobacco daily, and SLT less than daily, and 20.0% participants used
both smoked as well as SLT on less than daily basis.
Among SLT users, 5.6% reported increased tobacco use, 31.9%
reported no change, 33.3% reported decreased use, and 27.8%
reported no use of smoked tobacco during lockdown. Of the 53 SLT
users, 3.8% of users reported increased SLT use, 22.6% reported no
change, 43.4% reported decreased use, and 30.2% reported no use of
SLT during compared to before lockdown.
Among dual users, 4 (26.7%) reported no change in tobacco use
patterns. One (6.7%) participant reported the same smoking pattern
with increased SLT use. Two (13.3%) participants reported the same
smoking pattern with decreased SLT use during the lockdown. Two
(13.3%) participants reported an increase in both smoked and SLT use, 2 (13.3%) participants reported decreased use of both, and 2 (13.3%)
participants reported cessation of tobacco during the lockdown. An
increase in SLT use was also reported by 2 (13.3%) participants who
stopped smoking during the lockdown.
Table 2 depicts, availability of tobacco products during
the lockdown was significantly associated with a change in the
smoking pattern during lockdown. Participants reporting difficult/
no availability of tobacco during lockdown had higher odds of
showing a change in the pattern of tobacco usage during lockdown
(aOR=3.8; 95%CI=1.1-13.6). All of the smoked tobacco users who
reported tobacco to be unavailable during the lockdown reported
either a decrease in usage (18.2%) or stopped using smoked tobacco
(81.8%). More than half (57.1%) of those who reported tobacco to
be easily available during the lockdown reported the same usage as
before the lockdown. Change in family income during lockdown was
significantly associated with a change in SLT use patterns. Participants
who reported a decrease in family income had more odds of changing
their pattern of tobacco usage during lockdown (aOR=7.1; 95%CI
1.1-49.6).
During lockdown, among ten dual users who used tobacco daily,
4 (40.0%) participants reported no change in pattern. Two (20.0%)
participants reported increased use of both smoked and SLT. Two
(20.0%) participants reported decreased use of both smoked and
SLT. One (10.0%) participant reported the same smoking pattern,
but increased use of SLT, and another (10.0%) participant reported
decreased use of SLT with no change in smoking patterns. Among
2 participants who smoked tobacco daily and SLT less than daily,
both reported smoking cessation during lockdown, with cessation
of SLT in one participant and increased use of SLT in the other.
Among 3 participants who used both smoked and SLT less than daily,
1 participant reported cessation of both, one reported cessation of
smoking during lockdown and increased use of SLT, and 1 reported
no change in smoking but decreased use of SLT.
The most common reasons for decreased use of tobacco were
increased tobacco prices (41%), unavailability and difficult availability
of tobacco products (24%), and decreased income during the
lockdown (19%). In addition, a few participants reported change in
the pattern due to health conditions/ illness/ advised by a healthcare
provider (7%), fear of covid (4%), decreased or no cravings (4%), and
boredom/staying idle (2%), etc.
Among smoked tobacco users, 5.6% of users reported increased
tobacco use, 52.8% reported no change in tobacco use, 23.6%
reported decreased use, and 16.7% reported no use of smoked
tobacco after lockdown as compared to before the lockdown. Among
SLT users, 1.9% reported increased SLT use, 54.7% reported no
change, 30.2% reported decreased use, and 13.2% reported no SLT
use after lockdown compared to before lockdown. Among dual users,
3 (20.0%) participants continued to use tobacco with no change in
pattern as compared to before lockdown, 2 (13.3%) participants
reported an increase in the use of SLT, and 1 (6.7%) participants
reported a decrease in SLT use with no change in use smoked
tobacco. Five (33.3%) participants reported an increase in smoked
and SLT use, and 1 (6.7%) participant reported an increase in smoked
tobacco use with cessation of SLT. Two (13.3%) participants reported
a decrease in both smoke led and SLT, and 1 (6.7%) participant reported decreased smoking but no change in SLT use.
Table 3 shows that participants who reported continued tobacco
use during lockdown were more likely to report a change in the
pattern of tobacco use after lockdown (aOR 10.7, 95%CI: 2.6-43.5).
Half (50.0%) of the daily smoked tobacco users reported the same
usage after the lockdown. The majority (87.0%) of the users who
reported the same tobacco usage during the lockdown continued to
report the same after the lockdown. After the lockdown, those who
stopped using smoked tobacco during the lockdown, 40% reported
returning to the same usage pattern as before the lockdown. Among
those who reported decreased usage during the lockdown, half
(50.0%) reported decreased usage after the lockdown as well.
In comparison, about one-third (37.5%) reported a return to
similar usage as before the lockdown. The majority of the SLT users
native to Delhi reported the same usage pattern after the lockdown.
In contrast, more than half of the migrant users (52.4%) either
decreased using or stopped using after the lockdown. Migrants had
more odds of reporting a change in the pattern of SLT use (aOR: 12,
95%CI: 1.3-106). Among ten dual users who used tobacco daily, 2
(20.0%) participants continued to use tobacco with no change in
pattern compared to before lockdown. For a change in the pattern
of tobacco use after the lockdown, most of the participants (46.4%)
reported decreased or no cravings/habits as a common reason. Few
other participants reported change in the pattern due to increased
cravings/habit (10.1%), advised by a healthcare provider (8.1%),
decreased social gatherings (5.8%), and easy availability (5.8%).
Withdrawal symptoms during lockdown were assessed among
those who decreased or stopped using tobacco (smoked and/or
smokeless) during lockdown. Out of 140, 91 participants reported
decreased or no use of smoked and/or SLT. Of these 91 participants,
46.2% reported experiencing one or more of the withdrawal
symptoms included in the questionnaire, 53.8% experienced no
withdrawal symptoms during the lockdown.
Figure 1 shows that the most common withdrawal symptoms that
were observed were craving for tobacco (30.8%), irritability (28.6%),
and fatigue (23.1%). Few participants reported experiencing lack of
concentration (7.7%), constipation (6.6%), headaches (4.4%), hunger
(4.4%), insomnia (3.3%), cough (2.2%), nasal drip (1.1%), dizziness
(1.1%).
Among smokers, 12 participants had quit tobacco smoking after
lockdown. Of them, nine users had no plans of resuming tobacco
use, 2 participants planned to start again after lockdown, and one user did not know if they had any such plans when the interview was
conducted. None of the seven SLT users, who had quit after lockdown,
planned to resume tobacco use. Among dual users, only one user had
quit SLT use only and did not know if they had any plans to resume
SLT when the interview was conducted.
Of 140 study participants, 59 participants (42.1%) used alcohol
before the lockdown. Of them, 25 (42.4%) used alcohol daily, and 34
(57.6%) used alcohol less than daily. Units per week ranged between
<1- 84 units (median =10 units). During lockdown, 17 participants
(28.8%;11 daily, six less than daily users) reported no change in alcohol
use. Increased usage was reported by 5 participants (4 daily, one less
than daily users), decreased usage by 11 participants (5 daily, six less
than daily users), and 26 participants (5 daily, 21 less than daily users)
reported cessation of alcohol use during lockdown. Units consumed
per week ranged between <1-42 units (n=33). Of 42 (71.2%) alcohol
consumers who reported change in pattern of drinking during
lockdown, 35 (83.3%) also reported change in pattern of tobacco use.
After lockdown, 36 participants (61.0%;11 daily users and 25 less
than daily users) reported no change in alcohol use. Eight participants
(4 daily and four less than daily users) reported cessation of alcohol
use during lockdown. Units consumed per week ranged between
<1-63 units (n=51). Of 23 (39.0%) alcohol consumers who reported
change in pattern of drinking during lockdown, 14 (60.9%) also
reported change in pattern of tobacco use. During the study, seven
cannabis users were identified. Of the total participants, 6 used
cannabis daily, 1 used cannabis less than daily. During and after
the lockdown, among the daily users, 1 reported a decrease in use, 1
reported no change, and four users reported an increase in use during
the lockdown. During the study, only 1 participant reported the use
of smack with no change in use during or after lockdown. In addition,
study participants reported no other substance use.
Discussion
The COVID-19 pandemic and nationwide lockdown affected
the stock availability and price of tobacco and the pattern of tobacco
usage. It is the first such community-based study conducted in India to
assess the changes in patterns of tobacco usage during the lockdown.
The data was collected by the first author administered questionnaire
prepared after a thorough review of available literature. In addition,
change in patterns of tobacco use after the lockdown was lifted was
also studied, and associated factors were identified for the same. Thus,
the desired sample size was achieved despite the difficulties posed by
the pandemic, which provided the necessary power for the study.
The prevalence of change in the pattern of tobacco use during the
lockdown among the study participants was 71.4%. This was higher
as compared to the study conducted by Elias M. Klemperer et al. [4],
which reported a 58.6% change in smoking patterns (28.3% decrease
and 30.3% increase), and the study by SabujKanti Mistry et al. [12],
which reported 15.9% increase in tobacco use. These differences could
be because of differences in access to tobacco products, lockdown
restrictions, and socio-demographic variations between the study
populations. Difficult or no availability of smoked tobacco products
during the lockdown was significantly associated with a change in
the usage pattern of smoked tobacco during the lockdown (aOR=3.8;
95%CI=1.1-13.6). A decrease in family income during the lockdown
was significantly associated with a change in the pattern of usage of SLT during the lockdown (aOR=7.1; 95%CI=1.1-49.6). The difference
between changes in the pattern during the lockdown (71.4%) and
after the lockdown (49.3%) indicates the lockdown impacted tobacco
usage. Lifting of restrictions, along with the return to regular pricing
and availability of tobacco products, led to the return to old patterns
of tobacco usage after the lockdown. Restriction on shops selling
tobacco products in residential areas and raising prices of tobacco
products to make affordability difficult might aid in reducing tobacco
use. Yunfeng Shang et al. also recognised the reduced fiscal capacity
during the pandemics and their long term economic impact. There
effects are more pronounced in lower-middle income countries [13].
SARS outbreak in 2003 had proven to be catastrophic on economies
specially in Eastern Asia and Canada [13]. Widespread loss of jobs
was experienced during past epidemics and pandemics like Ebola
outbreak of 2014-15 in West Africa [14] and Liberia [13,15].
Withdrawal symptoms were reported by 46.2% of participants
who had decreased or stopped using tobacco during the lockdown.
The main reasons cited by the study participants for the change in
the pattern of tobacco use during the lockdown include increased
tobacco prices, unavailability of tobacco products, and a lack of
income. On the other hand, the leading reasons for the change in
the usage pattern after the lockdown include a decrease or absence
of craving, advice from healthcare professionals, and an increase in
craving. Similar reasons were quoted by the participants in the study
conducted by Himanshu A. Gupte et al. [11] in India.
These findings point to the directions in a policy change that
might effectively reduce tobacco usage not just during the lockdown
and pandemic but also as we slowly return to some form of normalcy
in our daily lives in the post pandemic period. It is also important
to note that limited support was available to the tobacco users who
experienced withdrawal symptoms during the lockdown. Limitations
of the study: The study design was cross-sectional; therefore, it was
not possible to prove cause and effect relationships. The study was
conducted six months after the gradual relaxation of lockdown
restrictions from the study area. This may have introduced some
recall bias regarding the availability and use of tobacco during the
lockdown. Underreporting the tobacco use of the various smoking
and SLT products due to social desirability bias could have affected
the study’s findings. The usage was self-reported and not verified
biochemically. Factors associated with a change in the pattern of
tobacco usage in dual users were only described but not analysed
due to the small sample of dual users. Data on second-hand smoke
exposure was not collected, which could be another vital avenue for
study due to the increased time spent indoors during the lockdown
and the pandemic as a whole. Due to small proportion of study
participants reporting use of alcohol and cannabis, its association
with change in pattern of tobacco could not be analysed for statistical
significance which could be an avenue for study in future researches.
Conclusion
Clear impact of lockdown on tobacco use is indicated by the
difference between change in tobacco use pattern during and after
lockdown in the study population. Lockdown restrictions led to
decreased income, increased prices and decreased availability of
tobacco, which were major reasons for changed pattern during
lockdown. Lifting of restrictions (post lockdown period) resulting in return to regular pricing, availability of tobacco products and
lack of support for those who experienced withdrawal symptoms,
caused return to old patterns of tobacco usage. The factors identified
in this study, if translated to policy changemight be effective in
reducing tobacco usage during the pandemic and beyond. This
recommended an effective implementation of Cigarettes and Other
Tobacco Products Act, increasing the taxes on tobacco, regulating
selling of tobacco by shop owners on licence basis making availability
limited and restricted, setting up effective tobacco cessation clinics in
community based care settings to manage withdrawal symptoms as a
part of essential care and provide appropriate support.
Funding
The study was funded and supported by World Health
Organisation.
Conflict of Interest
The authors declare that the research was conducted without any
commercial or financial relationships that could be construed as a
potential conflict of interest.
References
Citation
Yukti B, Kishore J, Jagdish K. Change in Patterns of Tobacco Use during Lockdown due to COVID-19. J Addiction Prevention. 2022;10(1): 8.