
Journal of Addiction & Prevention
Download PDF
 Figure 1: KRATOM LEAVES.
Figure 1: KRATOM LEAVES.
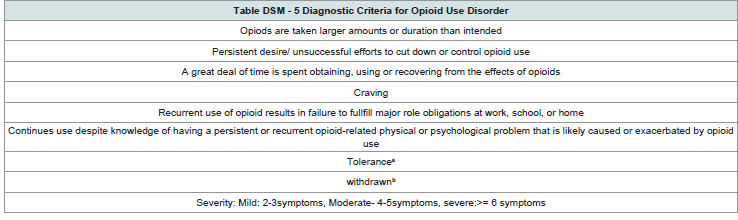 Table 1: DSM Criteria for opioid use disorder.
Table 1: DSM Criteria for opioid use disorder.
Review Article
Kratom- A Lethal Drug On The Rise
Oberbarnscheidt T1*, Miller NS2
1Department of Psychiatry, University of Pittsburgh, USA
2Professor of Psychiatry, Augusta University, current president of
Health Advocates PLLC, East Lansing, MI, USA
*Address for Correspondence: T. Oberbarnscheidt, MD PhD, Western Psychiatric Institute and Clinic, Department of Psychiatry, University of Pittsburgh, Pittsburgh, PA,
Email: Oberbarnscheidtt@upmc.edu
Submission: March 15, 2019
Accepted: March 26, 2019
Published: March 28, 2019
Copyright: © 2019 Oberbarnscheidt T. This is an open access article
distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
In Malaysia, Dutch botanist Pieter Korthals in 1831 first discovered
Kratom or Mitragyna speciosia. Kratom is derived from the Nitragyna
speciose korth, a tropical forest tree found in Malaysia, Thailand and
Myanmar. The trees’ leaves contain contain psychoactive opioid
compounds, consumed for thousands of years. Kratom contains
alkaloids that bind to opioid receptors, with an opioid drug structure.
Kratom induces euphoria, and in lower doses acts similar to a stimulant
by increasing energy, alertness, while in higher doses it induces sedation.
Kratom is purportedly used for anxiety, depression, inflammation, libido.
Importantly, given opioid activity, it suppresses opioid withdrawal. With
regular use, Kratom is associated with dependence and addiction.
Kratom is gaining increasingly popularity especially among the
young in the US population and is causing rising numbers of ER visits,
calls to poison control centers and even deaths related to multiple
causes.
There are currently very limited clinical studies available that
demonstrate safety and efficacy in humans. Kratom The FDA has not
approved Kratom for medical use, and publishes warnings regarding
its toxicity. Available information is mostly based on reports from
users or animal models. Case reports involving the use of Kratom are
concerning and alarming.
Kratom is classified as an herbal supplement and therefore easily
available to the user as it is sold in convenience stores, online or gas
stations. At this point, it is a dangerous drug with opioid activity, freely
available without controls for safety.
This article is a systematic review of literature on the current
available data on Kratom guided for physician and clinician education
and to raise awareness about Kratom as a substance.
Utilized sources were Pubmed, Ovid, Medline, PsychInfo, and
EMBASE.
Introduction
Kratom is a natural substance stemming from the Mitragyne
speciosia tree in Southeast Asia and has been used for thousands of
years [1,2]. In Asian countries it was used as a remedy for diarrhea,
pain, hypertension and cough. Also, it has been used in religious
ceremonies [1-3], (Figure 1).
Kratom can be ingested in various routes, traditionally chewed
but also smoked or strained in teas. The leaves have a very bitter taste
that can be masked by adding sugar or honey in juices or teas. As an
alternative, lemon juice can be added to facilitate the extraction of the
plant alkaloids. In Malaysia, the pill form is known as mandarin and
smoked in long bamboo pipes [1,4].
In Malaysia and Thailand Kratom was originally used to treat
intestinal infections, muscle pain, diarrhea or coughing. Other
indications were energy booster for workers to work in the fields in hot and humid climate [1,2].
The use of Kratom has now spread all over the world. In the US
it is mostly used for its stimulant effect, to enhance performance and
also to self-treat opioid withdrawal symptoms as a cheaper alternative
to Buprenorphine [5-8].
In recent years Kratom has become increasingly popular in
the US. About 40 million Americans are current using Kratom
recreationally [9]. Most nationally conducted surveys on drug and
alcohol use don’t ask about Kratom use, so the actual number of users
might be much higher, in particular in adolescents since it is easily
accessible and legal which might falsely be perceived as “safe” and
“just natural” [10].
Calls to US poison centers related to Kratom exposure increased
from 26 calls in 2010 to 263 calls in 2015 [11]. 36 deaths were reported
to the FDA in 2017. Kratom appears to be a drug increasingly used
in the US and published case reports and toxic effects are emerging
public health threat. Many health care providers have never heard
about Kratom as a substance, which bears a need for education and awareness [12].
Kratom’s pharmacological properties are similar to those of
opioids but unlike opioids it is not a federally regulated substance
[12]. There are increasing number of case reports with Kratom
intoxications and withdrawals that are challenging for the physicians.
Kratom is not a very commonly known substance and is also difficult
to detect as it does not cause positive findings in urine drug screens
[13]. The assessment relies on the history from the patient or specific
immune-assay tests [14]. The treatment can consist of symptomatic
treatment with Clonidine but also with Suboxone. There are several
cases reported of Kratom withdrawal and dependence [15].
According to the Drug Enforcement Agency Kratom is a legal
herbal product and available without restrictions in many states [12].
It is not a federally controlled substance and listed with the FDA as
“drug of concern”. Some states banned the sale and possession of
Kratom, those are Indiana, Tennessee, Wyoming, Florida, Alabama,
and Wisconsin [16].
Is Kratom a Substance that is Safe to be ordered off the Internet or
be purchased at the local convenience store?
Legal status:
Thailand scheduled preparations containing M. speciosa as early
as 1943. In 1979 the Thai government moved Kratom to schedule 5
of the Thai Narcotics Act which makes it illegal to buy, sell, import or
possess Kratom [17]. Malaysia tolerated Kratom until 2003 when it
placed the substance under the Poison Act, making the sale of Kratom
illegal [18]. Countries that still allow the sale and cultivation are
Indonesia which does sell Kratom on a large scale to North America
as well as European countries [19]. Denmark, Poland and Sweden
control the import of Kratom, but Germany and the US don’t control
the import of this substance on a federal level [20].
In the US, the Drug Enforcement Administration has placed
Kratom on the list of drugs with “chemicals of concern”. From a legal
standpoint, Kratom is regulated as an herbal product under US law
and US Food and Drug Administration and US Drug Enforcement
Administration (DEA) policies [12]. In 2016 the DEA attempted to
move Kratom to a schedule I substance, but public protest throughout
the US resulted in rejection of that plan. A letter was sent to Barack
Obama in September 2016 containing 130,000 signatures to support
the availability of Kratom for recreational use [21]. Within 2 month
the DEA withdrew the proposal to move Kratom to a scheduled
substance.
Six States have banned the distribution and sale of Kratom but
in the majority of states within the US, Kratom is available through
Internet or local convenience stores, smoke shops and even gas
stations [16]. Online, Kratom can be purchased as a plant itself or in
form of dried leaves or preparations in drinks [1,3].
Pharmacology of Kratom:
Origin and mechanism of action: Kratom (Mitragynia speciosa
korth) is a member of the Rubiaceae family, the same family that
includes coffee [1-3]. It is also known under the name Thang,
Kakuam, Thom, Ketum and Biak [22]. The fresh or dried leaves can
be chewed, smoked or consumed orally. It can be brewed with hot
water and made into syrup or powered and pressed into pill forms which are the most convenient form to distribute online [23].
The pharmacological effects of Kratom are dose dependent, small
doses 1-5 g of raw leaves can cause stimulant like effects, while higher
doses 5-15g can produce sedation and opioid like effect [24].
Animal studies and reports from users have shown that Kratom
does act as antipyretic, antidiarrheal, euphoric anti-depressant as well
as anxiolytics. It has shown to have properties as immunosuppressant,
appetite suppressant and anti-diabetic medication [25].
Kratom is a drug that acts in the central nervous system. It is very
lipophilic and easily crosses the blood brain barrier which causes the
onset of effects to occur quickly and potent [26].
Kratom contains 2 main alkaloids: mitragynine and
7-hydorxymitragynine (1-3). Both act as opioid agonist. It does bind
on mu-, delta as well as kappa opioid receptors [27]. However, the
classification of kratom as and “opioid” is based on its mechanism
of action and not on its molecular structure but more on it’s
pharmacological effects.
Mitragynine is 13 times more powerful than morphine however
the concentration is very low about 0.2% in Kratom. Twenty leaves
contain about 17 mg of mitragynine [28].
Mitragynine is also known as an adjunct to synthetic cannabinoids
such as K2 products [29]. There are also other pharmacological
active ingredients found 7-hydroxymitraggynine, paynantheine,
speciogynine and 20 other substance that are not well understood yet
[28].
The effects of Kratom on the central nervous system as well as
systemic effects can be inhibited or blocked by opioid antagonists
[27].
Kratom also acts as an antagonist on Calcium-channels, inhibiting
the neurotransmitter release from the vas deferens [30].
In addition is has agonist activity on alpha-2 receptors that
avert opioid withdrawal symptoms and may work similar to other
symptomatic treatments for opioid withdrawal for example Clonidine
[31].
The stimulant like effect of kratom is mostly contributed to the
antagonism on 5-HT2A receptors and it‘s effect is described very
similar to the effect of cocaine. Studies (Kumarnsit) have shown that
the dorsal raphe nucleus is a major binding site of Kratom in the
central nervous system [32].
The onset after chewing the leaves is about 5-10 min and lasts
approximately 2-5 hours.
The average clearance of mitragynine has been measures as 1.6
L/h, the elimination half-life is reported as 3.85 hours, and the total
clearance is 6.35 L/h /kg. In laboratory tests in rats, mitragynine
could still be detected in the rats 24 hours after oral administration
of Kratom [33].
The detection of Kratom requires specialized tests:
Ultra-high-performance liquid chromatography and highperformance
liquid chromatography- tandem mass spectrometry
methods have been successfully used in monitoring the major alkaloids and metabolites found in urine following Kratom use [34].
Kratom toxicity:
Kratom is associated with several severe toxic effects including
hypertension, nephrotoxicity, psychosis, seizures, and hepatotoxicity.
The risks of long-term use of Kratom are currently unknown. There
are no pharmacological or pharmacokinetic studies on humans
published or studies on drug interactions involving Kratom [35].
Kratom has shown in animal studies to affect the endocrine
system and suppress TSH similar to the effect of morphine on the
thyroid or stress related effects on the patient [36]. The liver toxicity
can range from mildly elevated liver enzymes to acute liver failure. A
case report from Kapp reported acute liver failure with jaundice and
pruritis following 2 weeks of ingestion of Kratom [37].
Also, neurotoxic effects of Kratom have been reported. During
the acute intoxication, there are cases of seizures reported from
individual case reports which also have been confirmed in animal
studies. Roche et al published a case report about a woman who
presented with a status epilepticus requiring intubation and ICU care
after ingestion of Kratom off the internet 24 hours prior [38]. The
exact mechanism is currently unknown. There are theories that the
mitragynines and their metabolites can lower the seizure threshold
similar to atypical opioids such as Tramadol or Meperidine. Kratom
has been shown to be neurotoxic in in vitro studies on neuronal cells.
The neurotoxicity can be reversed or prevented by administration of
Naloxone [38].
Respiratory depression is not reported consistently in studies and
appears to be dose dependent but death from overdoses have been
reported in the US as well in other countries [39]. The lethal dose of
Kratom in rats has been identified as 200 mg/kg. There is currently no
exact lethal dose known for humans. Overdoses have been reported
in the setting of long-term use and exposure as well as acutely after
first time ingestion [40].
Kratom when used during pregnancy has shown to be associated
with complications in pregnancy and has caused cases of neonatal
abstinence syndrome in the newborn [41].
Is Kratom an addictive substance?:
Kratom’s pharmacological properties and reported rewarding effects bear a significant risk of the development of an addiction.
Both the stimulant effect as well as the opioid like effect can lead to
compulsive use, use despite the negative consequences and regardless
or the decline in psychosocial functioning.
Animal studies in mice have shown that the rewarding properties
require an overtime dose increase to continue to have the same effect
[42]. Which would implicate the development of tolerance in these
mice after repetitive exposure of the substance? Individual reports
from Kratom users confirmed this presence of tolerance but there is
no controlled study in humans available to demonstrate this.
In early stages, the Kratom users are mostly able to fulfill their
work requirements and psychosocial functioning but the prolonged
use bears the risk of psychiatric problems and physical impairments
that make this difficult or impossible, which is very comparable to
other substances listed in the DSM V as substance use disorders.
Even though Kratom is not an acknowledge substance to cause
addiction according to DSM V it does fulfill the equivalent criteria
listed for opioid use disorder in some patients [43].
There are few case reports published that demonstrate the
development of addiction is possible, for example a 37-year old
teacher who tried Kratom for fibromyalgia and then consumed it
compulsively in increasing amounts, and despite the negative effect
on her marriage she was unable to cut back on the use without any
medical assistance and professional withdrawal treatment [44]. The
physiological and psychological dependence as well as tolerance and
withdrawal are also reported in case reports as well [45,46] Table 1.
Numerous reports have shown that the discontinuation of Kratom
causes moderate withdrawal that consists of symptoms nausea,
vomiting, diarrhea, lacrimation of eyes, rhinorrhea, restlessness, jerky
limb movements, agitation, insomnia, decreased appetite, aggression
as well as depression, anxiety similar to opioid withdrawal symptoms.
The length of withdrawal can be prolonged and potentially last for
more than a week [47].
In animal studies, the withdrawal symptoms could be induced by
administration of Naloxone and was shown to be reproducible [48].
The use of Kratom is more difficult to detect and monitor since
Kratom cannot be detected in regular drug screens. In order to measure mitragynine serum concentrations in rats and humans, technologies
high performance liquid chromatography with ultraviolet detection
is needed [49].
The current accessibility of Kratom makes the supply for
development of addiction easy as Kratom is cheap and easy to obtain:
Kratom is easily purchased through the internet and much cheaper
than heroin and methamphetamines. Kratom Extract 50x (5 grams)
cost $34.99, comparison the Ultra enhanced form is more expensive,
priced 5 grams $45.99. The price for an entire Kratom plant is around
$50 according to my internet searches.
Reported indications for Kratom use:
Kratom effects on humans are not well studied and understood
yet. Early reports were made by Wray in 1907 [50,51]. Most studies
that are available about Kratom are animal studies from rodents
(mice and rats).
Pain:
Animal studies have shown that Kratom prolongs the
latency to nociceptive or painful stimuli. In 2010 Sabetghadam et
al compared the anti-nociceptive effect of Kratom with Morphine
in rats and noticed a significant increase in pain response latency
by administering the “tail-flick- test” to the rats. Also, the group
noticed that the analgesic effect of Kratom can be potentiated by
co-administration of caffeine. This anti-nociceptive effect was
found with oral administration of Kratom as well as intra-cerebroventricularly.
In addition, it was noted that the effects of Kratom
on the pain perception could be blocked with co-administration of
Naloxone [52].
Other animal studies showed and anti-novice-time effect, which
is important in pain signaling and pain response of even 13 times
more potent than morphine [53].
An additional benefit from Kratom over morphine is that is also
acts as a muscle relaxant which has been shown in rats. It blocks the
nerve conduction as well as amplitude and action potential [53].
Inflammation:
Kratom carries some anti-inflammatory
properties: Kratoms major active compound, Mitragynine, inhibits
cyclooxygenase (COX)1 and 2 isoenzymes and in COX 2 mRNA
and protein expression as well as the release and production of
Prostaglandin PGE2 which is one of the strongest inflammatory
mediators [25].
In rodents, It has been shown that Kratom inhibits the early
phase of paw edema development in the first 3 hours after challenge.
In addition, it is found to inhibit the development of granuloma tissue
through particular macrophages as well as fibroblasts in the acutely
inflamed tissue. Kratom stimulates tissue repair, increases vascular
permeability in supports healing and immunity [25].
Kratom is found to have anti-microbacterial properties against
bacteria and has been tested against Salmonella typhi and Bacillus
subtilis which would explain why Kratom has been used traditionally
to treat gastro-intestinal infections [54].
Self-treatment of opioid withdrawal:
The first cases of opioid
substitution with Kratom were described by Low in the 1800’s [2].
Kratom is frequently used for opioid withdrawal symptoms. Blots
in the internet discuss and advise how to obtain and use it. There is no medical guided treatment for opioid withdrawal or treatment
prescribed by a physician [31].
Kratom’s compound Mitragynine is acting as an agonist on
postsynaptic alpha 2 receptors similar to Clonidine which is regularly
used for opioid withdrawal symptoms. Unlike Clonidine it does
improve withdrawal symptoms but at the same time potentiates the
opioid effect of the initially ingested opioid and also potentiates effects
from other sedative or hypnotic substances which does increase the
risk of sedation [31].
There are currently no studies available investigating the effect of
Kratom on opioid withdrawal symptoms in either human or animals.
Weight loss medication:
Animal studies in rats have shown that
acute as well as chronic administration lead to reduced food and
water intake and weight loss. Kratom influences the transit time of
water and food in the way of slowing the process down [55]. This
effect is mostly present in lower doses as Kratom does act similar as
a stimulant [24].
Other animal models show that Kratom does increase the glucose
uptake into the cell and increases the protein transporters for glucose
[55].
Unlike other substances that induce weight loss, it does not affect
the secretion or levels of cholecystokinin [56].
There are no human studies available that show the success rate of
weight loss or the associated long-term effects and adverse reaction.
There are many online forums of users that discuss the use of Kratom
for the indication of weight loss as a so called “health supplement”.
Kratom use for cognitive enhancement:
The use of Kratom
influences short-term learning in a positive way, so enhances shortterm
learning but does not improve any long-term consolidation of
learned material [57-59]. Further, animal tests have shown a delay
in passive avoidance learning. These effects of Kratom are facilitated
by Kratom’s inhibition of neuronal potentials in the hippocampus.
Compared to heroin users, chronic Kratom users have shown to
perform poorly on visual-spatial recognition tests [60].
Discussion
Kratom has been used in Asian countries as a natural remedy for
thousands of years. However, in the US, Kratom is becoming more
and more popular as a recreational drug for its stimulant as well as
opioid-like effect. The pharmacology and active ingredients are not
fully understood and available human research studies on Kratom are
very limited.
The increasing number of calls to the poison control centers
show, Kratom is not harmless even though it is a natural substance.
Opium is derived from a natural plant and poppy seeds as well and is
clearly a federally schedule 1 controlled substance. The term natural
should not be seen equal to harmless.
Should Kratom be available without any restrictions or should
Kratom become a schedule 1 substance controlled by the DEA or
should there be a Medical Kratom similar to the Medical Marijuana.
The current trend and failed attempt to federally control Kratom
bears risks for the US population.
Further studies are needed to completely understand Kratom and
its effects.
Research with Kratom as an herb is complicated due to the
inconsistencies in the substance which Kratom product should be
used and become evaluated? How should the standardization occur
in a substance with mixed compounds?
Another factor is that Kratom is not well known to many
physicians. Increased education is needed to provide improved
assessment of situation as well as improve treatment. Since Kratom
does not provide positive results in urine drug tests, the diagnosis
relies and the subjective history and specific questioning by the
physician.
Random screening tests for substance use disorders should
include questions regarding Kratom use. Also, it should be subject to
discussion, whether to include Kratom as a use disorder in the DSM
V.
Conclusion
Kratom is a substance that has been available for a long time
especially in the Asian areas that has certainly potent medical
properties. However more research and clinical studies are needed
to further investigate the properties of Kratom and toxicities. The
reported toxic effects of Kratom that have been confirmed in animal
studies are concerning.
The pharmacology of Kratom appears very fascinating how it
can act as a stimulant in low doses but then more as an opioid with
sedation in higher doses. Not all chemically active ingredients are yet
identified. There are many details to be learned about Kratom. Kratom
might have some medical properties but unlike FDA approved
medications, one sample is not the compatible with the next as the
concentrations of active ingredients are varying from plant to plant.
There are parallels to the current trend and use of Kratom and
Marijuana or so called “Medical Marijuana” these days. Those natural
substances are in the general public seen as harmless and without
major concerns. The legal availability makes Kratom and marijuana
socially acceptable and is also easily accessible for the adolescents.
There is no data available yet to look at the role of Kratom as a gateway
drug and link to other consecutive substances. This is partially the
case because only a very small fraction of kratom users reach out for
medical treatment and gets even identified. This has been a problem
among substance use disorders in general for decades. Public
education is a helpful tool to reach out and eventually prevent further
damage. The increasing number of case reports and contact with
patients in emergency rooms or poison control centers are alarming
to raise a concern to further regulate the availability of Kratom and
consider a change to federally controlled substance.
The current trend and associated risk as well as the economical
burden for medical care of Kratom users, missed worked days and
overall reduced psychosocial functioning are alarming.
With the current legal situation and tolerance to these natural
substances, Kratom and also Marijuana we are facing a trend in society
and a high degree of tolerance to allow and legalize impairment.
Alcohol as a licit substance shows similar impairment however is
easily detectable in breathalyzer tests and will cause consequences when used at workplace or hazardous situations for example traffic.
Kratom on the other hand does not show in standard drug screens or
tests. The current legal state allows everybody including bus drivers,
physicians and law enforcement officers to use it with all the negative
consequences.
More public awareness and physician education is needed
regarding Kratom. Until further and more detailed data on the
pharmacology and toxicity of Kratom in particular in humans is
available, stricter control and regulation would be safer for the US
population.
References
18.
European Monitoring Centre for Drugs and Drug Addiction. Kratom (Mitragyna speciosa) drug profile.
Citation
Oberbarnscheidt T, Miller NS. Kratom- A Lethal Drug on the Rise. J Addiction Prevention. 2019;7(1): 6.