
Research Article
*Address for Correspondence: Leanne Lester, Associate Professor, Health Promotion Evaluation Unit, University of Western Australia, 35 Stirling Hwy, Crawley WA, 6009, Australia; Tel: +61 8 6488 3842; Fax: +61 8 6488 1039; E-mail: leanne.lester@uwa.edu.au
Citation: Lester L, Midford R, Cahill H, Mitchell J, Ramsden R, et al. Cannabis and Harm Minimisation Drug Education: Findings from the Drug Education in Victorian Schools Study. J Addiction Prevention. 2014;2(1): 7.
Copyright © 2014 Lester L, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Addiction & Prevention | ISSN: 2330-2178 | Volume: 2, Issue: 1
Submission: 09 June, 2014 | Accepted: 04 July, 2014 | Published: 07 July, 2014
This research is part of a longitudinal efficacy study that followed a cohort of students from the start of year eight in 2010 (average age 13) to the end of year ten in 2012 (average age 15). The study was approved by Edith Cowan University’s and the University of Melbourne’s human research ethics committees. It was also approved by the Research Branch, Education Policy and Research Division of the Victorian Department of Education and Early Childhood Development. The intervention students received 10 lessons of the 18 lesson research-derived education programme during 2010, followed by eight lessons in 2011. The lessons, which were delivered by teachers, are described in Table 1. In both years the teachers delivering the classroom programme participated in intensive two-day professional training. This incorporated a summary of the evidence-base informing the programme and active sampling of each lesson activity. Emphasis was given to modelling and coaching in use of the participatory, skills-based and critical thinking pedagogy. No program lessons were scheduled in 2012. The control students received drug education lessons usually provided by their school. These varied considerably from school to school, as no standard curriculum was specified.
Talking to parents: Students were asked to indicate how often they talked to their parents about cannabis in the past 12 months. Response choices were: Never; once or twice; 3-4 times; 5-11 times; and 12 times or more.
Communication with parents
The average number of times intervention students talked to their parents about cannabis increased from Baseline to Post1 by 50%, from Baseline to Post2 by 100% and from Baseline to Post3 by 67% for intervention students and from Baseline to Post1 by 0%, from Baseline to Post2 by 20% and from Baseline to Post3 by 20% for control students (Table 2). The increase in talking with parents by intervention students was significantly greater at Post1 (p=0.001) and Post2 (p=0.001) than for the control students [Table 3].
 Cannabis lessons remembered
Cannabis lessons remembered
The proportion of intervention students who recalled receiving more than one lesson on cannabis increased from 12.9% at Baseline to 48.4% at Post1, 59.6% at Post2 and 24.6% at Post3 (table 2). The proportion of control students who recalled receiving more than one lesson on cannabis increased from 9.1% at Baseline to 14.9% at Post1, 44.4% at Post2 and 13.4% at Post3. After taking into account recall of cannabis lessons at Baseline, gender, SES category and region, intervention students recalled receiving significantly more cannabis education than control students at Post1 (p<0.001) and Post2 (p<0.001) and significantly less education at Post3 (p<0.001) (table 4). Attitudes
Attitudes
The attitudes of students towards cannabis issues in both the intervention and control groups were highly responsible at Baseline, with intervention and control students scoring 19.5 and 19.7 respectively out of a possible 25 (table 2). Attitude scores increased by 10.3% at Post1, 10.3% at Post2 and 14.9% at Post3 for intervention students and 5.1% at Post1, 9.6% at Post2, and 9.6% at Post3 for control students. There was a significant difference between groups in the change of attitudes from Baseline to Post1 with intervention students having a greater increase in responsible attitudes than control students (p=0.001) [table 3].
Used cannabis
The proportion of students who had used cannabis in the past 12 months increased from 2.8% at Baseline, to 3.4% at Post1, 7.7% at Post2 and 11.2% at Post3 [21](table 2). The increases for intervention and control students were quite similar. From Post1, males had slightly higher prevalence than females, and metropolitan students’ slightly higher prevalence than rural students. There was no significant difference between groups in the increase in the number of cannabis users at any time point [table 4].
Frequency of cannabis use
The frequency of cannabis use in the past 12 months increased at Post1 for intervention and control students and then dropped at Post2 for intervention students and increased for control students, with a 9.1% increase from Baseline to Post3 for intervention students (mean Baseline= 20.8, Post1= 32.3, Post2= 26.3, Post3 = 22.7) and a 219% increase for control students (mean Baseline=9.8, Post1= 26.8, Post2= 32.6, Post3 = 31.3) (table 3). The frequency of cannabis use for control students increased significantly at Post3 (p=0.030) compared to intervention students.
Cannabis harms
Cannabis harms experienced by intervention student cannabis users during the previous 12 months increased by 2.7% from Baseline to Post1, decreased by 10.8% from Baseline to Post2 and decreased by 18.9% from Baseline to Post3(table 2). Cannabis harms experienced by control student cannabis users during the previous 12 months increased by 64.1% from Baseline to Post1, by 28.2% from Baseline to Post2, and 28.2% from Baseline to Post3 (table 3). The difference in harms experienced by intervention and control students was significantly different at Post2 (p=0.030) and Post3 (p=0.008) [Table 3].
Cannabis and Harm Minimisation Drug Education: Findings from the Drug Education in Victorian Schools Study
Leanne Lester1*, Richard Midford2, Helen Cahill3, Johanna Mitchell4 Robyn Ramsden5David R Foxcroft6and Lynne Venning7
- 1Health Promotion Evaluation Unit, University of Western Australia, 35 Stirling Hwy, Crawley WA, 6009, Australia
- 2Charles Darwin University,Ellengowan Drive, Casuarina NT, 0810, Australia
- 3The University of Melbourne,Level 5, 100 Leicester Street,Carlton VIC, 3010, Australia
- 4Curtin University,Kent Street, Bentley WA, 6102, Australia
- 5Royal Far West,19-21 South Steyne Street, Manly NSW, 2095, Australia
- 6Oxford Brookes University,Gipsy Lane, Oxford OX3 0BP, United Kingdom
- 7Victorian Department of Education and Early Childhood Development, PO Box 5, Dandenong VIC, 3175, Australia
*Address for Correspondence: Leanne Lester, Associate Professor, Health Promotion Evaluation Unit, University of Western Australia, 35 Stirling Hwy, Crawley WA, 6009, Australia; Tel: +61 8 6488 3842; Fax: +61 8 6488 1039; E-mail: leanne.lester@uwa.edu.au
Citation: Lester L, Midford R, Cahill H, Mitchell J, Ramsden R, et al. Cannabis and Harm Minimisation Drug Education: Findings from the Drug Education in Victorian Schools Study. J Addiction Prevention. 2014;2(1): 7.
Copyright © 2014 Lester L, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Addiction & Prevention | ISSN: 2330-2178 | Volume: 2, Issue: 1
Submission: 09 June, 2014 | Accepted: 04 July, 2014 | Published: 07 July, 2014
Abstract
Aims: To evaluate the effectiveness of an integrated harm minimisation focused school drug education programme in terms of reducing cannabis use and harm.Design and Methods: A cluster randomised controlled trial of the 18 lesson Drug Education in Victorian Schools (DEVS) drug education programme was undertaken with students during years eight and nine (13 and 14 years of age respectively), with follow up in year ten (15 years of age). The programme covered all drugs, employed a harm minimisation approach that used participatory, critical thinking and skills based teaching methods, and engaged parental influencethrough home activities. Twenty-one secondary schools in Victoria, Australia, were randomly allocated to receive the DEVS programme (14 schools) or the drug education usually provided by their schools (7 schools). In relation to cannabis, communication with parents, lessons remembered, responsible attitudes, whether used, frequency of use and associated harms were measured.
Results: In comparison to controls, there was a significantly greater increase in the intervention students’ communication with parents about cannabis recall of cannabis lessons received, and responsible attitudes towards cannabis. While there were no significant differences between the two study groups in relation to the proportion of cannabis users, the increase in level of use by intervention students was significantly less and they experienced a lesser increase in associated harms.
Conclusion: A harm minimisation focused school drug education programme reduced the level of cannabis use and associated harm. This supports harm minimisation education as an effective prevention strategy for school students.
Keywords
Cannabis; Education; Schools; Students; Harm minimisationIntroduction
Cannabis is the most widely used drug in Australia after tobacco and alcohol [1]. In a recent study of Australian adolescents it was estimated that 11% aged 12-17 have used cannabis in their lifetime, 9% have used cannabis in the last 12 months, 3% in the last month, and 1% in the last week [1]. Prevalence of cannabis use increases with age, with an earlier Australian study estimating past year cannabis use at 2% at age 12, increasing to 20% at age 16 [2]. A more recent longitudinal study estimated past year use at 8% at age 15, increasing to 30% at age 19 [3]. Cannabis use has also been found to be more prevalent among males than females [3], and significantly higher in rural adolescents compared to urban adolescents [4].While the overall prevalence of past year cannabis use has been declining in Australia since the late 1990s, heavy patterns of daily use are prevalent among 14-19 year old adolescents [5]. Cannabis exposure is associated with a range of harms, with adolescents a vulnerable group at high risk of suffering adverse consequences. Cannabis use in adolescence is associated with lasting consequences on cognition, an increased risk of psychosis and depression, increased risk of neuropsychiatric disorders, illicit drug taking, and increased likelihood of cannabis dependence [6-9]. Associations exist between cannabis use and truancy, fighting, and poorer educational and occupational outcomes [9,10]. Scholes-Balog and colleagues [3] in their longitudinal study of 800 Victorian young people aged 15-19, explored the rates of a range of self-reported cannabis-related social harms. This study found the most prevalent self-reported cannabis related harms were anxiety and depression, and that while the rate of cannabis use increased with age, the rates of cannabis-related social harms remained fairly consistent as the participants aged [3].
While abstinence or delayed onset is almost universally the goal of school drug education in the United States (US), in Australia most school drug education seeks to prevent harm in accordance with the harm minimisation framework of the National Drug Strategy [11]. Harm minimisation includes abstinence as a preventative strategy [12]: it is more broadly relevant to students [13] and does not increase up take or level of use [14,15]. A recent comparison study of rates of lifetime and current alcohol, tobacco, and cannabis use in Washington State (US) and Victoria (Australia) showed greater use of cannabis in Washington State, causing the authors to speculate the abstinence approach to drug use within the US did not provide a greater protective effect than the harm minimisation approach to illicit drug use implemented within Australia [4]. The Drug Education in Victorian Schools (DEVS) programme was designed to provide young people with the practical knowledge and skills to enable them to prevent or minimise the harms most likely to be encountered due to drug use, both their own, and that of others. Eighteen lessons were provided over two years to a cohort of junior secondary school students. The program took an integrated approach to all drug use, both licit and illicit, employed participatory, critical thinking and skill-based teaching methods and engaged parental influence through home activities. This paper uses longitudinal data to compare adolescents who received the DEVS programme with the control group who received the drug education normally provided by their schools.
The aim of this research is to evaluate the effectiveness of the DEVS programme in terms of cannabis prevention. The study measured the difference between the intervention and control groups in communication with parents about cannabis, lessons remembered about cannabis, and responsible attitudes towards cannabis, as these can be important influences on cannabis use [16,17]. However, the primary outcomes sought by the programme were reductions in cannabis consumption and associated harm as well as avoidance of use. Accordingly, consumption patterns and associated risk/harm were measured, with specific hypotheses that intervention students will: consume less cannabis and experience less harm associated with their use of cannabis.
Materials and Methods
Design
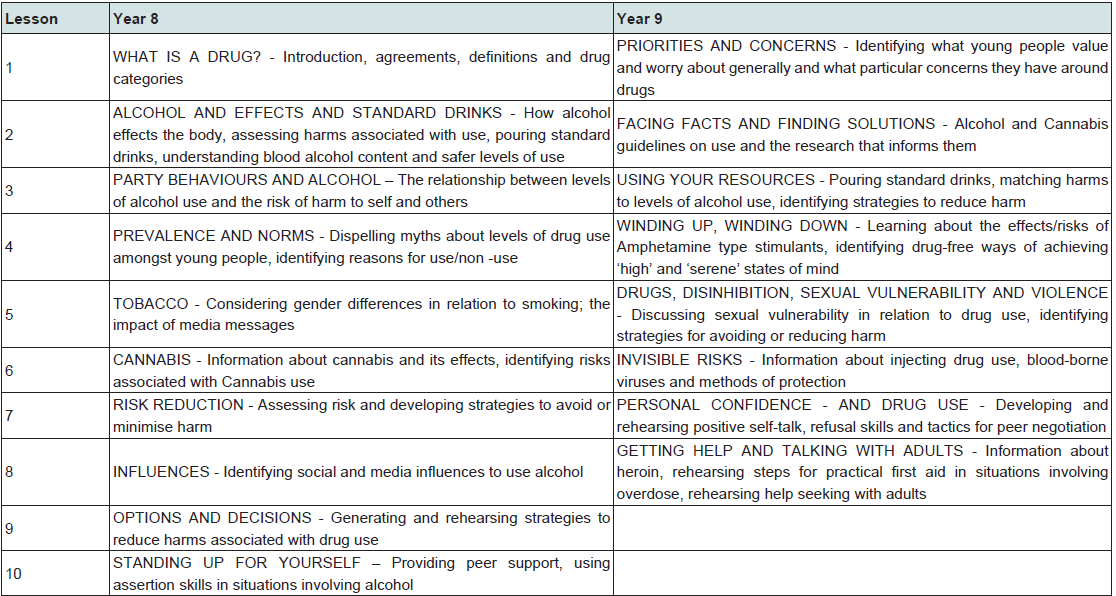
Table 1: Year eight and year nine lesson plans.
Sampling and data collection
Twenty-one Victorian government secondary schools were recruited to the study on a voluntary basis at the beginning of 2010, and allocated to metro/regional location and high/low socioeconomic (SES) strata to approximate the proportion of Victorian secondary schools in each category. SES allocation was made using the Department of Education and Early Childhood Development’s (DEECD) Student Family Occupation (SFO) index for 2010. Schools within each strata were then randomly allocated to intervention or control conditions. A piece of paper, folded to conceal the name of a school was drawn out of one container, while a similarly folded piece of paper, designating the research condition was drawn out of another container [18]. Subsequently, schools were further partitioned into high, medium and low socio-economic strata. This was done to better align with DEECD’s school SES categories. One intervention school, with 44 participating students at Post1, withdrew from the second year of the study in 2011 because they did not have the resources to implement the programme.Written active consent was sought from the 2700 year eight students in the 21 participating schools and their parents. Of this total population 1752 or 64.9% agreed to participate in the research. At Baseline, 1161 usable surveys were returned by intervention students and 585 by control students. Six Baseline surveys were excluded as unreliable because all responses to the questions on either alcohol, smoking, cannabis or other drug use and harm were uniformly in the highest category. This was considered a strong indication that these students had not reported their true behaviour, but simply reported maximum possible values. At Post3 a slightly smaller proportions of usable surveys were returned by intervention (n=621, 53.5% of Baseline returns) than control students (Post3 n=345, 59.0% of Baseline returns) (Figure 1). This is partly an artefact of the intervention school withdrawal.
Measures
Lessons: Students were asked to recall the number of lessons concerning cannabis they had received at school over the past year. The question was phrased in the same manner as that asked as part of the 2008 national survey of secondary school students’ use of alcohol [2] to enable comparison. Response choices were: Not even part of a lesson; part of a lesson; one lesson; and more than one lesson.
Attitudes: The cannabis responsible attitude scale was the sum of agreement with five statements in relation to using cannabis. Higher scores represented more responsible attitudes. The cannabis responsible attitude scale was the sum of five harm items relating to the social and health consequences of cannabis use. The internal consistency of the scale was measured during the pilot phase, using the Cronbach’s alpha test (alpha=0.548, p<0.001) [19].
Cannabis Use: Students were asked to indicate if they had used cannabis in the past 12 months, and if so, the frequency of their use.
Harms: The cannabis harms scale was the sum of five harm items relating to the social and health consequences of cannabis use. The internal consistency of the scale was measured during pilot phase, using the Cronbach’s alpha test (alpha=0.891, p<0.001) [19].
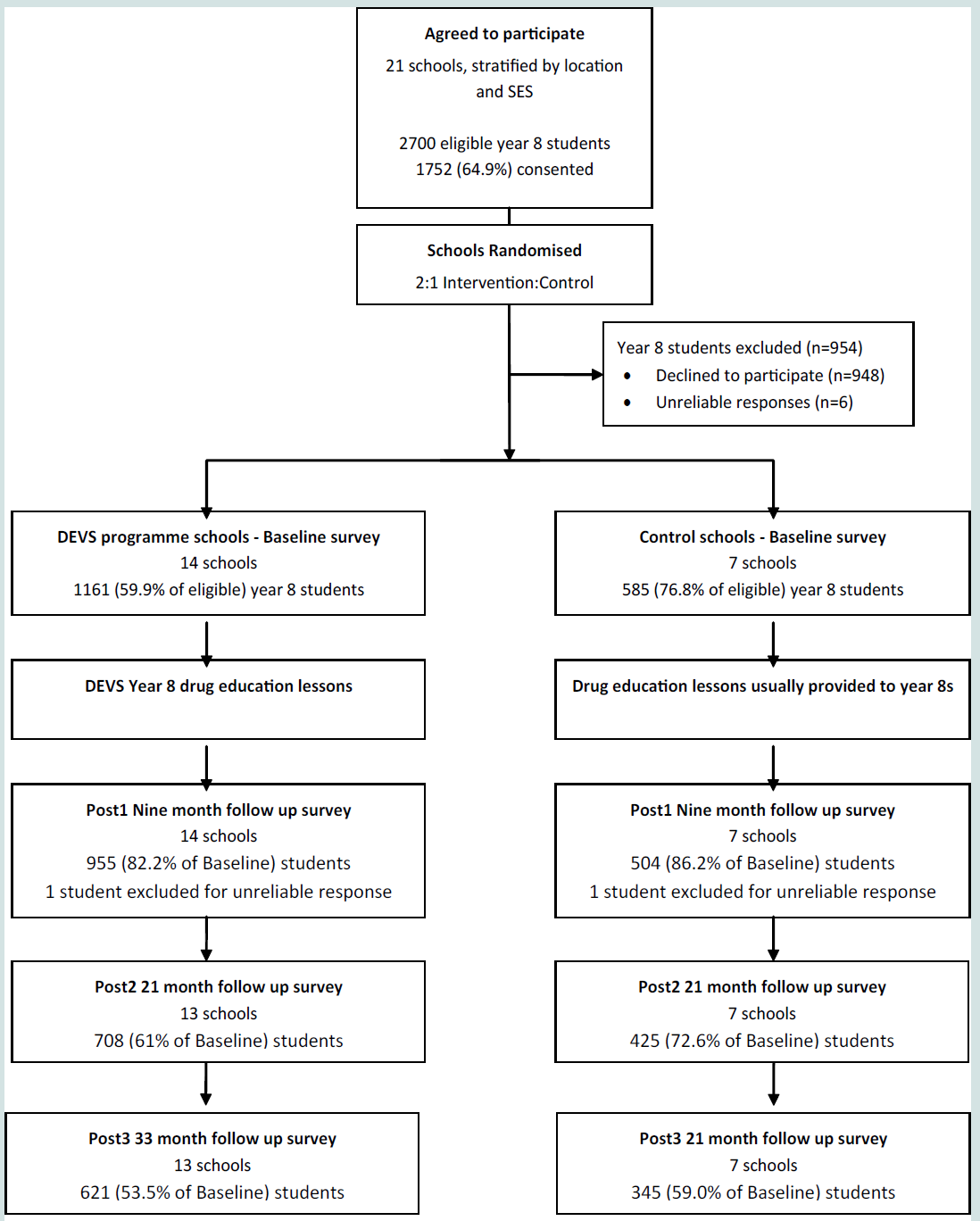
Figure 1: Flow chart illustrating the recruitment and participation of schools and students in the full Year8 and 9 drug education programme.
Statistical Analysis
Analyses were conducted using STATA v 13 and SPSS v 21. Separate multi-level regression models were fitted with Post independent variables modelled as a function of the study condition, gender, region, SES and Baseline variables to adjust for any Baseline differences between the intervention and control groups. A random intercept was included in each model to account for the clustering of students within schools. All students were included in linear regression models which were used to determine differences between intervention and control groups in relation to talking to parents about cannabis, cannabis attitudes, frequency of use and cannabis harms. An ordinal logistic regression model was used to determine differences between groups in the number of cannabis lessons recalled. Logistic regression models were used to determine differences between groups as to whether the students had used cannabis.Results
The average number of times intervention students talked to their parents about cannabis increased from Baseline to Post1 by 50%, from Baseline to Post2 by 100% and from Baseline to Post3 by 67% for intervention students and from Baseline to Post1 by 0%, from Baseline to Post2 by 20% and from Baseline to Post3 by 20% for control students (Table 2). The increase in talking with parents by intervention students was significantly greater at Post1 (p=0.001) and Post2 (p=0.001) than for the control students [Table 3].
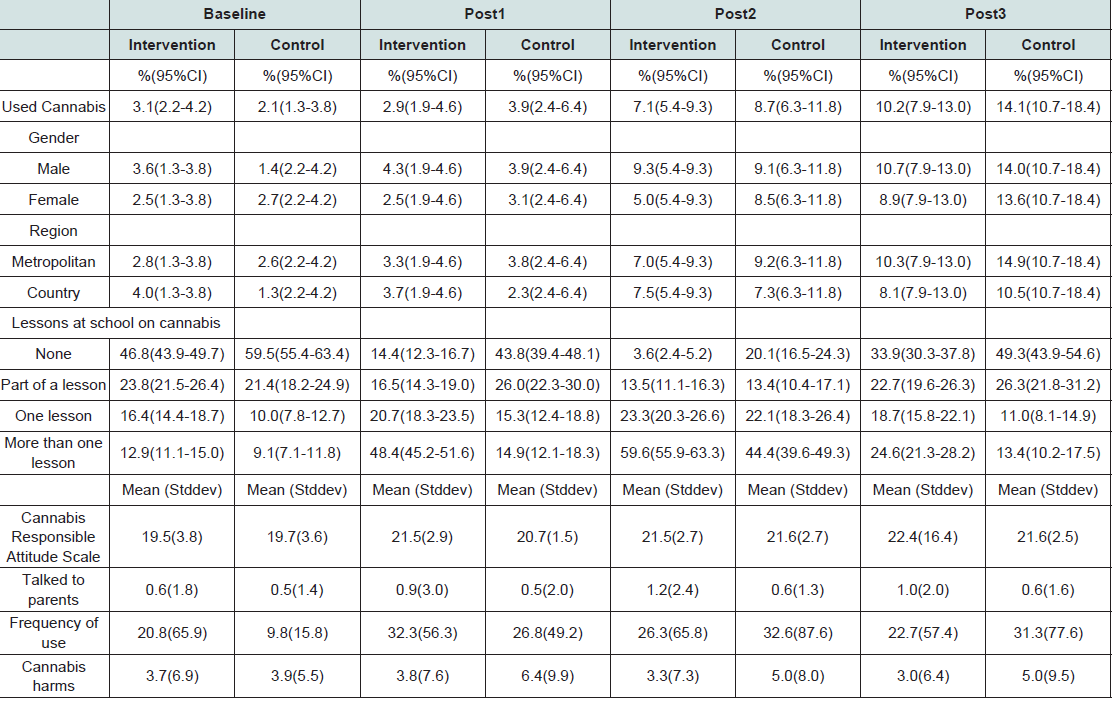
Table 2: Year eight and year nine lesson plans.
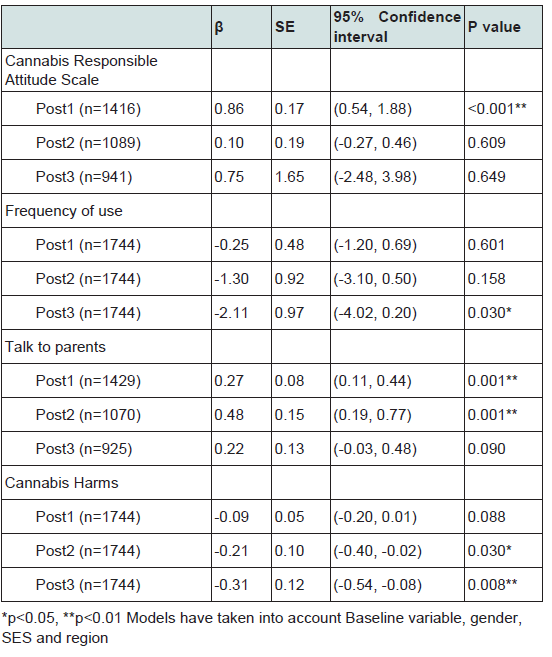
Table 3: Multi-level linear regression models for the intervention group by time period.
The proportion of intervention students who recalled receiving more than one lesson on cannabis increased from 12.9% at Baseline to 48.4% at Post1, 59.6% at Post2 and 24.6% at Post3 (table 2). The proportion of control students who recalled receiving more than one lesson on cannabis increased from 9.1% at Baseline to 14.9% at Post1, 44.4% at Post2 and 13.4% at Post3. After taking into account recall of cannabis lessons at Baseline, gender, SES category and region, intervention students recalled receiving significantly more cannabis education than control students at Post1 (p<0.001) and Post2 (p<0.001) and significantly less education at Post3 (p<0.001) (table 4).
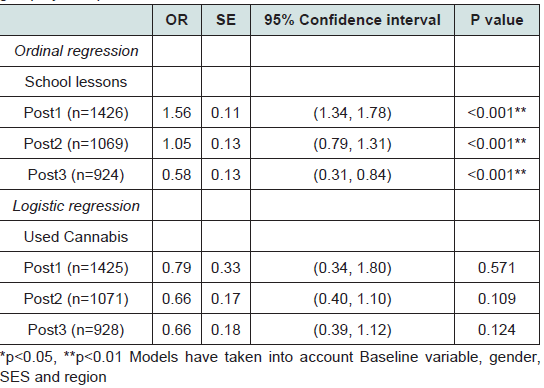
Table 4: Multi-level ordinal and logistic regression models for the intervention group by time period.
The attitudes of students towards cannabis issues in both the intervention and control groups were highly responsible at Baseline, with intervention and control students scoring 19.5 and 19.7 respectively out of a possible 25 (table 2). Attitude scores increased by 10.3% at Post1, 10.3% at Post2 and 14.9% at Post3 for intervention students and 5.1% at Post1, 9.6% at Post2, and 9.6% at Post3 for control students. There was a significant difference between groups in the change of attitudes from Baseline to Post1 with intervention students having a greater increase in responsible attitudes than control students (p=0.001) [table 3].
Used cannabis
The proportion of students who had used cannabis in the past 12 months increased from 2.8% at Baseline, to 3.4% at Post1, 7.7% at Post2 and 11.2% at Post3 [21](table 2). The increases for intervention and control students were quite similar. From Post1, males had slightly higher prevalence than females, and metropolitan students’ slightly higher prevalence than rural students. There was no significant difference between groups in the increase in the number of cannabis users at any time point [table 4].
Frequency of cannabis use
The frequency of cannabis use in the past 12 months increased at Post1 for intervention and control students and then dropped at Post2 for intervention students and increased for control students, with a 9.1% increase from Baseline to Post3 for intervention students (mean Baseline= 20.8, Post1= 32.3, Post2= 26.3, Post3 = 22.7) and a 219% increase for control students (mean Baseline=9.8, Post1= 26.8, Post2= 32.6, Post3 = 31.3) (table 3). The frequency of cannabis use for control students increased significantly at Post3 (p=0.030) compared to intervention students.
Cannabis harms
Cannabis harms experienced by intervention student cannabis users during the previous 12 months increased by 2.7% from Baseline to Post1, decreased by 10.8% from Baseline to Post2 and decreased by 18.9% from Baseline to Post3(table 2). Cannabis harms experienced by control student cannabis users during the previous 12 months increased by 64.1% from Baseline to Post1, by 28.2% from Baseline to Post2, and 28.2% from Baseline to Post3 (table 3). The difference in harms experienced by intervention and control students was significantly different at Post2 (p=0.030) and Post3 (p=0.008) [Table 3].
Discussion
The findings of this study support a harm minimisation approach in school drug education that applies to cannabis use. The DEVS intervention, based upon harm minimisation principles, recognises the need for practical relevance, with success interpreted not as reduced use or abstinence alone, but by a reduction in the level of harm experienced from drug use [20]. The DEVS program curriculum is well-grounded in evidence-based research: Knowledge and skills training; the use of interactive activities; and role playing exercises which involve realistic drug scenarios, all features in the DEVS intervention. The program also places particular emphasis on teacher fidelity and on family communication activities as the evidence suggests these factors can increase the effectiveness of an intervention [21,22].The intervention had an impact in terms of the likely precursors to behaviour change. For example, exposure to, and understanding of, salient drug and alcohol information increases the likelihood of behaviour change. The intervention students remembered receiving more lessons specifically about cannabis than the controls at Post1 and Post2. The lessons recalled by the intervention students dropped significantly below the controls at Post3, reflecting that no DEVS program cannabis lessons were given in year three. Data collected from the same study and reported previously also found that intervention students were more knowledgeable about drug use issues, including cannabis use [23-25].
At baseline, both the intervention and control students held very responsible attitudes towards cannabis use. After the first year of the DEVS program, the increase in responsible attitudes towards cannabis use was significantly greater in the case of intervention students. Intervention students also talked more frequently to their parents about cannabis over the two years of the DEVS program than control students. However these positive changes disappeared over time. An explanation for the drop off in intervention students talking to parents could lie in program delivery and the accompanying home tasks ceasing in the third year of the study. The disappearance of a difference in responsible attitudes towards cannabis use is, however, more likely due to a ceiling effect than program influence. The estimate of reliability of the cannabis responsible attitude scale was low for this study.
Overall cannabis use prevalence figures were found to be similar to an earlier study of Australian secondary school students, with prevalence increasing with age [2]. In this study, students who received the study intervention were no less likely to take up cannabis use, but neither were they more likely to take it up. Intervention students were also no more likely to use more frequently than control students at Post1 and Post2, similar to other harm minimisation education programmes which did not increase experimentation among intervention students [14]. However by Post3, intervention students actually used less frequently than control students, even though no program drug education was provided in that year. This suggests the education program had a progressive effect that only produced change of sufficient magnitude in the small population of cannabis users after three years.This result runs counter to conventional wisdom that the effects of drug education decay over time [26].
The intervention was successful in reducing the number of cannabis harms experienced.Cannabis users in the intervention group reported experiencing fewer harms throughout, and following, the two-year harm minimisation focused education programme here as cannabis users in the control group, who received the normal drug education provided by their school, experienced more harms over the life of the study. This suggests the harm minimisation message held relevance for those who did choose to use cannabis, and led to more positive decision-making in relation to use. It has been argued that a harm reduction framework for cannabis prevention that addresses the social context of use will be more effective than those that focus on individual risk factors and choices [27]. Such a framework can focus on the minimisation of harm associated with drug use, and measure the success of such initiatives in terms of their effectiveness in reducing the impact of drug use on individuals and society, rather than by prevalence of use alone [28]. School drug education programs using this method engage students in thinking about the potential for harm, and provide opportunities for students with decision making skills to develop strategies to reduce or prevent or reduce harm [29]. Therefore, while abstinence is acknowledged as the best way to minimise harm associated with drug use, it is likely to be unrealistic in some circumstances and may be counter-productive if it does not provide opportunity for students to engage in their own critical thinking about the risks of drug use [12]. While it has been feared that the harm minimisation approach may reduce the impact of the abstinence message for drug use, the evidence suggests that this has not been the case. For example, the Smoking Cessation for Young People project in Western Australia, which employed a harm minimisation approach to tobacco smoking, found that there was no increase in experimentation amongst recipients of the program compared with a traditional abstinence approach [14].
A harm minimisation approach can also minimise potential harms arising from the use of multiple drugs. For example, a recent study has found that the combination of cannabis and alcohol, even under the legal blood alcohol limit in Australia of 0.05, significantly impaired driving ability [30]. Therefore, it is valuable for users to have knowledge of the effects of combined drug use in order to reduce harm associated with use [30]. The inclusion of cannabis within a multi-substance drug education program is supported by research which highlights the relationship between licit alcohol use and illicit cannabis use, with very few cannabis users having never consumed alcohol [31]. It is also argued that many of the strategies and skills learned in drug education are transferable and applicable for various types of drug use [32]. Therefore, a multi-substance education program can be particularly useful for simultaneously addressing risk factors common to all drug use. Such a program also has the significant benefit of easy incorporation into an already crowded school curriculum. This is viewed as a particular strength of a comprehensive drug program such as the DEVS curriculum.
Despite the illegal status of cannabis in Australia, harm minimisation strategies can work alongside, rather than in opposition to, policing activities. For example, reducing the frequency of use is seen as a vital goal for minimising harm arising from cannabis and is recognised and explicitly endorsed within the Australian National Drug Strategy [11]. Therefore, a preventative, school drug education program that employs a harm minimisation framework, which has the potential to address both the minor and the harms associated with cannabis, and is more effective than a traditional abstinence-focused program, is not only supported by research, but is also politically feasible within the current Australian National Drug Strategy.
References
- Welfare AIoHa (2010) National drug strategy household survey report. Canberra: AIHW.
- White V, Smith G (2009) Australian secondary school students use of tobacco, alcohol, and over-the-counter and illicit substances in 2008.Melbourne: Cancer Council Victoria.
- Scholes-Balog KE, Hemphill SA, Patton GC, Toumbourou JW (2013) Cannabis use and related harms in the transition to young adulthood: A longitudinal study of Australian secondary school students. J Adolesc 36:519-527.
- Coomber K, Toumbourou JW, Miller P, Staiger PK, Hemphill SA, et al. (2011) Rural adolescent alcohol, tobacco, and illicit drug use: a comparison of students in Victoria, Australia, and Washington State, United States. J RuralHealth 27: 409-415.
- Roxburgh A, Hall WD, Degenhardt L, McLaren J, Black E, et al. (2010) The epidemiology of cannabis use and cannabis related harm in Australia 1993– 2007. Addiction 105: 1071-1079.
- Schneider M (2008) Puberty as a highly vulnerable developmental period forthe consequences of cannabis exposure. Addict Biol : 253-263.
- Patton GC, Coffey C, Carlin JB, Degenhardt L, Lynskey M, et al. (2002) Cannabis use and mental health in young people: Cohort study. BMJ 325:1195-1198.
- Patton GC, Coffey C, Lynskey MT, Reid S, Hemphill S, et al. (2007) Trajectories of adolescent alcohol and cannabis use into young adulthood. Addiction 102: 607-615.
- Fergusson DM, Horwood LJ, Beautrais AL (2003) Cannabis and educational achievement. Addiction 98: 1681-1692.
- McCrystal P, Percy A, Higgins K (2007) Frequent cannabis use among 14/15 years old in Northern Ireland. Drug Alcohol Depend 88:19-27.
- Ministerial Council on Drug Strategy. National drug strategy 2010-2015. Canberra: Commonwealth of Australia, 2011 8 August, 2012. Report No.
- Lenton S, Midford R (1996) Clarifying ‘harm reduction’? Drug and Alcohol Review 15: 411-413.
- Marlatt GA, Witkiewitz K (2010) Update on harm-reduction policy and intervention research. Annu Rev Clin Psychol 6: 591-606.
- Hamilton G, Cross D, Resnicow K, Shaw T (2007) Does harm minimisation lead to greater experimentation? Results from a school smoking intervention trial. Drug Alcohol Rev 26: 605-613.
- McBride N, Farringdon F, Midford R, Meuleners L, Phillips M. (2004) Harm minimization in school drug education: final results of the School Health and Alcohol Harm Reduction Project (SHAHRP). Addiction 99: 278-291.
- Bremner P, Burnett J, Nunney F, Ravat M, Mistral W (2011) Young people, alcohol and influences: a study of young people and their relationship with alcohol. York: Joseph Rowntree Foundation.
- Miller Day M (2008) Talking to youth about drugs: What do late adolescents say about parental strategies? Family Relations 57: 1-12.
- Midford R, Cahill H, Foxcroft D, Lester L, Venning L, et al. (2012) Drug Education in Victorian schools (DEVS): the study protocol for a harm reduction focused school drug education trial. BMC Public Health 12:112-119.
- Midford R, Cahill H, Ramsden R, Davenport G, Venning L, et al. (2012) Alcohol prevention: what can be expected of a harm reduction focused school drug education programme? Drugs: Education, Prevention, and Policy 19:102-110.
- Midford R (2006) Looking to the future: Providing a basis for effective school drug education. In Midford R. and Munro G . (eds.) Drug education in schools: searching for the silver bullet. IP Communications, Melbourne.
- Rohrbach L, Gunning M, Sun P, Sussman S (2010) The project Towards No Drug Abuse (TND) dissemination trial: implementation fidelity and immediate outcomes. Prev Sci 11: 77-88.
- Durlak JA, DuPre EP (2008) Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol 41: 327-350.
- Midford R, Cahill H, Ramsden R, Davenport G, Venning L, et al. (2012) Alcohol prevention: What can be expected of a harm reduction focused school drug education programme? Drugs: education, prevention and policy 19: 102-110.
- Midford R, Mitchell J, Lester L, Cahill H, Foxcroft D, et al. (2014) Preventing alcohol harm: Early results from a cluster randomised, controlled trialin Victoria, Australia of comprehensive harm minimisation school drug education. Int J Drug Policy 25:142-150.
- Mitchell J, Midford R, Cahill H, Ramsden R, Lester L, Venning L, et al. (2013) Smoking prevention: what benefits are indicated by a pilot school drug education programme that focuses on minimising harm? Int J Health Promo Edu 51: 95-107.
- Flay BR (2000) Approaches to substance use prevention utilizing school curriculum plus social environment change. Addict Behav 25: 861-885.
- Hyshka E (2013) Applying a social determinants of health perspective to early adolescent cannabis use – An overview. Drugs: Education, Prevention, and Policy 1-10.
- Midford R (2010) Drug prevention programmes for young people: where have we been and where are we going? Addiction 105:1688-1695.
- Hall W, Fischer B (2010) Harm reduction policies for cannabis. In: Rhodes T, Hedrich D, editors. Harm Reduction: evidence, impacts and challenges. Luxembourg: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA).
- Downey LA, King R, Papafotiou K, Swann P, Ogden E, et al. (2013) The effects of cannabis and alcohol on simulated driving: Influences of dose and experience. Accid Anal Prev 50: 879-886.
- Leatherdale S, Ahmed R (2010) Alcohol, marijuana, and tobacco use among Canadian youth: do we need more multi-substance prevention programming?J Prim Prev 31: 99-108.
- Stead M, Stradling R (2010) The role of schools in drug education and wider substance misuse prevention. In: Warwick I, Aggleton P, Dennison C, editors. Promoting health and well-being through schools. Oxon: Routledge.