
Review Article
*Address for Correspondence: Hakan Ozturk, Department of Urology, School of Medicine, Sifa University, Izmir-Turkey, Tel: +902324460880; Fax: +902324460770; E-mail: drhakanozturk@yahoo.com.tr
Citation: Saracoglu M, Zengin T, Ozturk H, Genc M. Female Genital Mutilation/Cutting Type 4. J Androl Gynaecol. 2014;2(4): 5.
Copyright © 2014 Saracoglu M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Andrology & Gynaecology | ISSN 2332-3442 | Volume: 2, Issue: 4
Submission: 03 November, 2014 | Accepted: 16 December, 2014 | Published: 15 December, 2014

Female Genital Mutilation/ Cutting Type 4
Musa Saracoglu1, Tarik Zengin1, Hakan Ozturk1* and Mine Genc22
- 1Department of Urology, School of Medicine, Sifa University, Izmir-Turkey
- 2Department of Gynecology, School of Medicine, Sifa University,Izmir-Turkey
*Address for Correspondence: Hakan Ozturk, Department of Urology, School of Medicine, Sifa University, Izmir-Turkey, Tel: +902324460880; Fax: +902324460770; E-mail: drhakanozturk@yahoo.com.tr
Citation: Saracoglu M, Zengin T, Ozturk H, Genc M. Female Genital Mutilation/Cutting Type 4. J Androl Gynaecol. 2014;2(4): 5.
Copyright © 2014 Saracoglu M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Andrology & Gynaecology | ISSN 2332-3442 | Volume: 2, Issue: 4
Submission: 03 November, 2014 | Accepted: 16 December, 2014 | Published: 15 December, 2014
Abstract
World Health Organization has defined four types of Female genital mutilation/cutting. Type 4 defines all types of non-medical intervention on female genitals. This includes piercing, tattoos, pricking, scarring, incision and cauterization of female genitals. Gishiri incision is a special form of female genital incision practiced in Niger and Nigeria and carries significance as a preventable cause of urinary fistula.Practices like piercing and tattooing of female genitals has become a subject of significance around the world. In addition to having important complications, these practices also have social, ethical and psychological significance because they are also practiced on individual under the age of 18. Necessity of labioplasty interventions on individuals in adolescent period is also subject to discussion.
It is expected that non-governmental organizations will show the same level of effort they showed for eradication of Type 1, 2 and 3 of female genital mutilation/cutting also for eradication of Type 4 interventions. The first step towards expected in this direction is education and rising awareness of the society, starting with the young people.
Keywords
Female genital mutilation; Female genital cutting; Piercing; TattooIntroduction
According to the report published in 1991by World Health Organization (WHO) declared that the practice recognised as female circumcision is a violation of basic human rights and does not describe exactly what is done hence it is not synonymous with male circumcision but a form of mutilation. “Female genital mutilation” (FGM) was has since been recognized internationally however practicing communities prefer the term cutting because it is unbiased [1]. Some authors have posited it would be more accurate to name this practice as “Female genital cutting” (FGC). Some other authors have preferred to combine these two terms and use the term “Female genital mutilation/cutting” (FGM/C) [2,3]. For the purpose of this review, the term FGM/C shall be used.WHO has defined four types of FGM/C.? Among these, Type 1, 2 and 3 are related to a type of intervention practiced for many years and known as female circumcision in the old literature [1,4]. FGM/C Type 4 is used to define other interventions made for non-medical reasons [1].
FGM/C Type 1, 2 and 3 maintains its significance as a serious health problem. It is estimated currently 140 million women have been subjected to FGM/C Type 1, 2 or 3, and 3 million people are added to this number annually [1,5].
FGM/C Type 4 defines non-medical interventions on female genitals, including piercing, pricking, tattoo, incision, labioplasty and cauterization. The fact that a significant part of these interventions are practiced outside medical institutions limits the accessible epidemiological data on the subject.
WHO has declared all four types of FGM/C practice as unnecessary and harmful? The Organization has observed that a zero tolerance policy should be applied against these practices and such practices should be eradicated from the society [1,6].
Even though WHO has observed the need for measures against all four types of FGM/C, almost all public and non-governmental organizations focus on Type 1, 2 and 3 practices and spend their efforts on eradication of these interventions [5,7]. On the other hand there is a decided lack of focus on Type 4 interventions and this subject is generally overlooked.
Today the number of piercing and tattoo studios around the world is on the rise. More and more people undergo FGM/C Type 4 interventions. Application of these interventions on genital areas, and especially the fact that they are also practiced on children under the age of 18, adds significance to the subject.
FGM/C Type 1, 2 and 3 interventions are generally practiced on female children between the ages of 4 and 10, in an age period where they are not capable of comprehending the importance of the matter [1,5,6]. On theother hand, Type 4 interventions are generally practiced on mature age groups, with knowledge and consent of the subject person. This is another important dimension of the subject matter.
This evaluation aims to point out the importance of this subject by reviewing the information regarding FGM/C Type 4 practices.
Due to varied nature of practices the subject will be reviewed under the sub headings of female genital piercing, female genial pricking, female genital tattooing, female genital incision, labioplasty and other types of intervention.
Female Genital Piercing
The terms “piercing” or “body piercing” define placement of a special material on the body by a piercing action disrupting integrity of the skin [8]. The materials placed on the body during piercing intervention are referred to as “piercing jewellery”.Piercing applications are made on almost all regions of the body, starting with ears, lips, nose and tongue. In addition, nipples and genital areas are also included among the regions subjected to piercing [8].
Piercing applications existed among Ancient Egypt, Aztec, Inca, Maya and Far East civilizations. It is known that this practice has spread among western societies after translation and publication of Kama Sutra, a sexual doctrine book, in English [9]. The reference that men should have their genital organs pierced to enjoy sexual relations in the second section of this book have probably increases practice of piercing applications in western societies. After men, women also followed in having piercings done.
Female genital piercings are applied on clitoris, labia minor, labia major and preputium clitoris. The most widely practiced female genital piercing is the horizontal clitoris piercing. The piercings placed on labium can include one side or both sides. The recovery period for clitoris piercings is 4 to 8 weeks, while it is between 1 to 3 months for labia minor, and 1 to 2 months for labia major [8,10].
Piercing jewellery should be of a quality which will not cause infectious or allergic reactions in the body when placed on the body. Therefore inert, non-toxic metals are preferred. The most widely used metals include steel, gold, niobium, titanium and alloys of these. The nickel content in the gold or gold plated piercing jewellery items can cause allergic reactions [8,10].
Other qualities required in piercing jewellery include being easily removable (especially in case of trauma and radiological examinations), having a smooth surface, being suitable for sterilization in autoclave, and being easy to clean [8].
Piercing jewelleries of various shapes and sizes are used on different regions of the body. Essentially there are three types of piercing jewellery. These are ring, loop and rod type jewelleries. Loop type jewelleries can include models varying between a slightly arching shape to almost complete circle.
In some countries placement of piercings is practiced by trained professionals at special studios. Piercing placement and tattooing practices are generally performed by the same people. In many developing countries piercing placement is not defined as a profession. Therefore it can be difficult to regulate this type of businesses.
Even though there is a principal against application of genital piercings to people under the age of 18, the studies show that genital piercings are applied on underage girls [11-14].
Table 1 lists the genital piercing complications seen on women. General complications include the piercing complications that can be seen on any region of the body. Gynecological complications are seen in case of genital piercing [15-18].
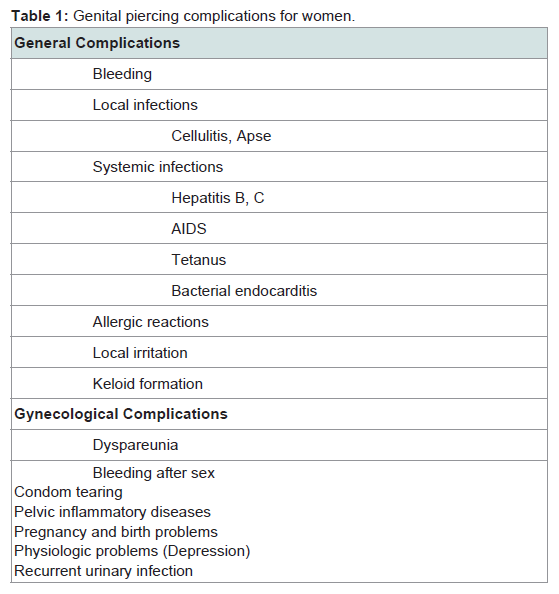
Table 1: Genital piercing complications for women
Female Genital Pricking
Female genital pricking is single or multiple perforation(s) on clitoris preputium applied without any excision [19]. It is a type of intervention performed as a symbolic practice by some tribes in Africa and South America [20]. Some researchers working toward rehabilitation of FGM/C Type 1, 2 and 3 have considered pricking as an alternative [21-24]. However, since this practice is also not condoned by the WHO, this has stayed as an idea and did not find any application.Female Genital Tattooing
Tattooing is an intervention performed by injecting various inks under the dermis layer of the skin. Other than camouflage of disease in case of some diseases like vitiligo and alopecia, it is largely used for purposes of decoration [25].The classic monochrome tattoo inks are gradually being replaced by multi-coloured inks. Various additives are used to obtain coloured tattoo inks. These additives generally consist of metal salts. The mercury and cadmium salts used for this purpose carry a significant toxicity risk. Even though these materials are not listed by any official authority, none of them are allowed for subcutaneous application. Printer inks and automobile paints are also used to obtain coloured inks [25].
Swelling due to granulomatous reaction and rashes caused by allergic reaction are foremost unwanted reactions related to tattooing [26]. It is reported that inks including azo pigment can have carcinogenic effects when exposed to sunlight and laser light [27,28].
Various histological effects are observed on regions with tattoos. These include pseudo-lymphoma, lichenoid, granulomatous reaction, moderate acanthosis, scleroderma-like changes, pseudoepitheliomatous hyperplasia and allergic contact dermatitis [29-37].
Infectious complications of tattooing are similar to piercing, most importantly including Hepatitis B, Hepatitis C, HIV, tuberculosis and tetanus. In addition, purulent infections also have a significant place [25,33].
Female Genital Incision
Female genital incision is generally practiced for medico-legal reasons (kindly explain this) or in scope of traditional practices. Medico-legal situations can come into light in scope of various forensic incidents. Examples of traditional and cultural practices include Gishiri incision performed among some the Hausa’s in Northern Nigeria and Southern Niger [38].This traditional practice is common especially among Hausa’s living in the rural parts of these countries. It involves making a longitudinal incision in the anterior vaginal wall using a sharp cutting tool. It is done in case of difficult or painful sexual intercourse, vaginal stenosis or difficult birth. Most of the time, the incision is not limited to anterior vaginal wall but also extends to the urethra and bladder resulting to urinary fistulae. Gishiri incision accounts for 5.68 to 18 % of the urinary fistulae seen in these regions [38-41].
In addition to being a FGM/C Type 4 intervention, Gishiri incision also carries significance as a preventable reason of urinary fistulas. It is believed that it will be possible to forestall this practice by various educational programs [40,41]. Also common among this group is ‘Angurya cut’ which is described as scraping of the vaginal orifice.
Labioplasty
World Health Organization considers any non-medical intervention on external genitals of female individuals under FGM Type 4 category. Under this light, labioplasty interventions performed outside medical reasons should also be considered under this category. Labioplasty involved excision and reconstruction interventions performed on labia minor. Even though it is reported to be made by aesthetic and functional concerns, it is also expressed that the practice is not supported by evidence-based findings [42,43].Grover points out that the level of increase in this intervention is not acceptable and the society has to be educated on this subject. Grover reports that the number of labioplasty patients in Australia increased by five times in the five year period following 1994, pointing out that this increase also included patients under the age of 25, and seeks answers to the medical reasons, if any, for these interventions. In conclusion the author underlines that this type of intervention is no different than FGM. He expresses that he cannot understand why those who react to FGM do not object to labioplasty [44].
Grover’s study on histological evaluation of labia minor tissue samples obtained from labial fusion operations, Schober et al. report that these tissue samples have a rich content of nervous structures and a special vascular structure. The authors points out the risk of ausing problems in sexual arousal and satisfaction stages due to removal of these tissues. They also point out that tissue replacements in this region will cause different sensory effects [45].
In their study conducted in USA with participation of 750 surgeons, Mirzabeigi et al. report that 2255 labioplasty operations in total were performed in a 24 months period, which means 7.37 operations per surgeon in the said 24 months period [42]. However, based on the information provided by the surgeons on their internet sites, it is seen that even a single surgeon can be involved in hundreds of labioplasty operations. This leads us to believe that there is a disproportionality between labioplasty operations performed in daily practice and reporting of such operations.
Other Attempts
Although it is not emphasized in literature, WHO takes the situations such as stretching, burning, cauterizing, scratching into FGM Type 4 category.WHO defines four types of the FGM/C attempts? FGM/C Type 1, 2 and 3 are used in order to express the attempt, known as female circumcision in old terminology. FGM/C Type 4 refers to any kind of non-medical attempt, applied on woman genitals.
The attempts on the woman genitals such as drilling, stretching, burning, cauterizing, scratching and incising within FGM/C Type 4 category are the attempts concerning a few number of people in the world. Being among these attempts and a special kind of incision on woman genitals, Gishiri incision is applied in Niger and Nigeria locally. It is significant from the point of the preventable reason of urinary fistulas. It is hoped that this application can be ended with the training activities in these regions.
The attempts on the woman genitals such as piercing, tattoo and labioplasty application within FGM/C Type 4 category are the attempts, being applied commonly and concerning a large number of people in the world.
Piercing and tattoo applications are applied in the same workplace generally. Many people take the one of these two applications. There are workplaces, serving these applications, in many countries. These workplaces are called as studio as well as the operators of these applications call themselves artists. Piercing and tattoo applications are defined as a profession in many countries gradually. It is considered that there are some potential problems related to these workplaces, whose numbers are increasing all over the world.
One of the significant potential problems during piercing and tattoo applications is whether the sterilization conditions are provided in an ideal level or not. The primary reason of infectious complications is not to care of this aspect adequately. One of the other problems is whether the person, who will take a piercing or tattoo application, is informed about the risks adequately an in detail or not. If correct information about the risks of this application is provided, probably some people can give up this attempt.
The most important problem related to piercing and tattoo applications is that these applications are made on genital areas of the persons under age 18. It is remembered that any attempt on genital areas of the persons in adolescence period is significant from the legal, social, ethical and physiological point. Furthermore, piercing or tattoo applications on genital areas of the persons under age 18 must have various meanings.
Savaser et al. include 287 high school students in a study in Turkey. They reported that the rate piercing application is 16.6% and the rate of thinking to take application is 14.7%. It was reported that piercing was applied on 348 areas and 12 of them were genital area in a study group, whose age average is 17 [11].
Owen et al reported 33% of piercing and 3% of genital piercing in a study, that they had included 595 college students in USA [12].
Cegolon et al. determined that 20% of the students had piercing and 25% of the students, having not piercing, thought to take a piercing application in a study, that they had included 4277 college students in Italy. It was stated in the study of Cegolon that 56% of the piercing-having-students are under age 18 [13].
In the study of Cossio et al. in Chile, 1329 adolescents, whose average ages were 15, were evaluated and it was reported that there was tattoo at the rate of 1.7% and piercing at the rate of 30.6 % [14].
The relationship between high-risky behaviors and piercing and tattoo was evaluated. Cossio et al. reported that high-risky behaviors such as usage of cigarette, alcohol, addictive drugs and existence of criminal records and early sexual relation are pointedly in higher level on the persons, having piercing or tattoo [14].
In the study of Owen et al. it was reported that there are highrisky behaviors in higher level on those, having four tattoos or more and eight piercings or more, and no matter how many it is, on those, having tattoo or piercing on the genital area [12].
These findings point that the tendency to tattoo and piercing indicates the tendency to high-risky behaviors as well. This point should not be ignored while training all the society, especially the adolescents.
One of the attempts, required to take into consideration, is labioplasty. Performing this application on young people more frequently causes hesitance about the medical necessity. Grover put emphasis on this aspect and reported that he could not understand the organizations, criticizing about FGM/C Type 1, 2 and 3, however,making no attempt on this aspect [44]. The most significant difference of labioplasty, resembling to FGM type 2 and 3, is that it is applied upon the demand of the patient. However, in what reason the young people demand this application is a matter of debate.
Consequently, the attempts within type 4 group according to the WHO classification have significant risks from the point of human health. WHO offers “zero tolerance” against FGM/C for these attempts? Therefore, the required precautions should be taken against this kind of applications and the great efforts should be made in order to prevent them. Training the society, mainly the young people, should be the starting point.
References
- WHO (2011) An UpdateonWHO’sWork on Female Genital Mutilation (FGM),Progress Report, World Health Organization, Geneva, Switzerland
- JBerg RC, Underland V, Odgaard-Jensen J, Fretheim A, Vist GE (2014) Effects of Female genital cutting on physical health outcomes: a systematic review and meta-analysis. BMJ Open 4: e006316
- Berg RC, Denison E (2012) Does female genital mutilation/cutting (FGM/C) affect women’s sexual functioning? A systematic review of the sexual consequences of FGM/C. Sex Res Soc Pol 9: 41-56.
- Saraçoglu M, Öztürk H (2014) Female Circumcision. Androl Gynecol Curr Res 2:2.
- UNICEF (2013) Female genital mutilation/cutting: a statistical overview and exploration of the dynamics of change. UNICEF Publications 184.
- WHO (2008) Eliminating female genital mutilation: an interagency statement. Geneva: World Health Organization
- E Edouard (2013) International efforts on abandoning female genital mutilation. Afr J Urol 19:150-153.
- Armstrong ML, Caliendo C, Roberts AE (2006) Genital piercings: what is known and what people with genital piercings tell us. Urol Nurs 26: 173-179.
- Burton RF, Rau SR, Spellman JW (translators) (1992) The Kama Sutra of Vatsyayana Chapter 2. London: Barnes Et Nobel.
- Armstrong ML, Kelly L (2001) Tattooing, body piercing, and branding are on the rise: perspectives for school nurses. J Sch Nurs 17: 12-23.
- Savaşer S, Balcı S, ÖzdinçerArslan S, Metreş Ö (2009) Liseöğrencilerindepi rsinguygulamaları. İ.Ü.F.N. Hem. Derg 17: 69-75.
- Owen DC, Armstrong ML, Koch JR, Roberts AE (2013) College Students With Body Art: Well-Being or High-Risk Behavior? J Psychosoc Nurs Ment Health Serv 51: 20-28.
- Cegolon L, Miatto E, Bortolotto M, Benetton M, Mazzoleni F, et al. (2010) Body piercing and tattoo: awareness of healt related risks among 4,277 Italian sekondary school adolescent. BMC Public Health 10: 73.
- Cossio ML, Giesen LF, Araya G, Pérez-Cotapos ML (2012) [Association between tattoos,piercings and risk behaviors in adolescents]. Rev Med Chil 140:198-206.
- Meltzer DI (2005) Complications of body piercing. Am Fam Physician 72: 2029-2034.
- Wilcox RR (1981) Sexual behavior and sexually transmitted disease patterns in male homosexuals. Br J Van Dis 57: 167-169.
- Gokhale R, Hernon M, Ghosh A (2001) Genital piercing and sexually transmitted infections. Sex Transm Infect 77: 393-394.
- Hounsflied V, Davies SC (2008) Genital piercing in association with gonorrhoea, chlamydia and warts. Int J STD AIDS 19: 499-500.
- Abdulcadir J, Margairaz C, Boulvain M, Irion O (2011) Care of women with female genital mutilation/cutting. Swiss Med Wkly 140: w13137.
- Budiharsana M (2003) Female circumcision in Indonesia: extent, implications and possible interventions to uphold women’s health rights. Population Council (Jakarta).
- Johnsdotter S, Essen B (2010) Genitals and ethnicity: the politics of genital modifications. Reprod Health Matters 18: 29-37.
- Lambelet Coleman D (1998) The Seattle Compromise: Multicultural Sensitivity and Americanization. J Duke Law 47: 717-783.
- Catania L, Abdulcadir OH (2003) Si può proporre un rito alternativo, ticamente e legalmente accettabile, in una strategia di lotta efficace contro le MGF? Toscana Medica.
- Policy Statement (2010) Ritual Genital Cutting of Female Minors. Pediatrics 125: 1088-1093.
- Ortiz AE, Alster TS (2012) Rising concern over cosmetic tattoos. Dermatol Surg 38: 424-429.
- Straetemans M, Katz LM, Belson M (2007) Adverse reactions after permanent-makeup procedures. N Engl J Med 356: 2753.
- Jemec GB (2010) Comment on: tattooing of skin results in transportation and light-induced decomposition of tattoo pigments. Exp Dermatol 19: 61-62.
- Cui Y, Spann AP, Couch LH, Gopee NV, et al. (2004) Photodecomposition of Pigment Yellow 74, a pigment used in tattoo inks. Photochem Photobiol 80:175-84.
- Blumental G, Okun MR, Ponitch JA (1982) Pseudolymphomatous reaction to tattoos. Report of three cases. J Am Acad Dermatol 6: 485-488.
- Clarke J, Black MM (1979) Lichenoid tattoo reactions. Br J Dermatol 100:451-454.
- Vagefi MR, Dragan L, Hughes SM, Klippenstein KA, et al. (2006) Adverse reactions to permanent eyeliner tattoo. Ophthal Plast Reconstr Surg 22: 48-51.
- Verdich J (1981) Granulomatous reaction in a red tattoo. Acta Derm Venereol 61: 176-177.
- Bagley MP, Schwartz RA, Lambert WC (1987) Hyperplastic reaction developing within a tattoo. Granulomatous tattoo reaction, probably to mercuric sulfide (cinnabar). Arch Dermatol 123: 1560 -1561.
- Kluger N, Mathelier-Fusade P, Moguelet P (2009) Scleroderma-like reaction restricted to the red parts of a tattoo. Acta Derm Venereol 89: 95-96.
- Goldstein N (1967) Mercury-cadmium sensitivity in tattoos. A photoallergic reaction in red pigment. Ann Intern Med 67: 984-989.
- Balfour E, Olhoffer I, Leffell D, Handerson T (2003) Massive pseudoepitheliomatous hyperplasia: an unusual reaction to a tattoo. Am J Dermato Pathol 25: 338-340.
- Kaur RR, Kirby W, Maibach H (2009) Cutaneous allergic reactions to tattoo ink. J Cosmet Dermatol 8: 295-300.
- Yola AI (2011) Yankan Gishiri (Salt Cut). Intl J Obst Trauma 1: 1.
- Tahzib F (1985) Vesicovaginal fistula in Nigerian children. Lancet 2: 1291- 1293.
- Tahzib F (1983) Epidemiological determinants of vesicovaginal fistulas. Br J Obstet Gynaecol 90: 387-391.
- Tukur J, Jido TA, Uzoho CC (2006) The contribution of gishiri to vesicovaginal fistula in Birnin Kudu, Northern Nigeria. Afr J Urol 12: 121-125.
- Mirzabeigi MN, Moore JH Jr, Mericli AF, Bucciarelli P, et al. (2012) Current trends in vaginal labioplasty: a survey of plastic surgeons. Ann Plast Surg 68:125-134.
- Lynch A, Marulaiah M, Samarakkody U (2008) Reduction labioplasty in adolescents. J Pediatr Adolesc Gynecol 21: 147-149.
- Grover S (2009) Female genital mutilation. J Paediatr Child Health 45: 614- 615.
- Schober J, Cooney T, Pfaff D, Mayoglou L (2010) Innervation of the labia minora of prepubertal girls. J Pediatr Adolesc Gynecol 23: 352-357.