
Advances in Diabetes & Endocrinology
Download PDF
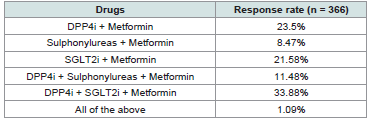 Table 1:Distribution of responses on the preferred initiation therapy in newly
diagnosed T2DM individuals with cardiovascular risk
Table 1:Distribution of responses on the preferred initiation therapy in newly
diagnosed T2DM individuals with cardiovascular risk
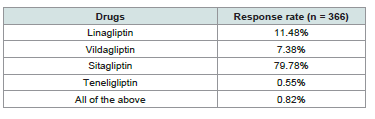 Table 2:Distribution of responses on the most preferred DPP4i for T2DM individuals with cardiovascular risk
Table 2:Distribution of responses on the most preferred DPP4i for T2DM individuals with cardiovascular risk
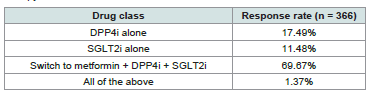 Table 3:Distribution of responses on the preferred add-on class of drug in the
management of T2DM patients uncontrolled with sulphonylureas + metformin
therapy
Table 3:Distribution of responses on the preferred add-on class of drug in the
management of T2DM patients uncontrolled with sulphonylureas + metformin
therapy
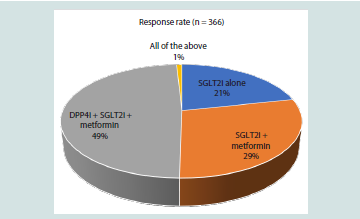 Figure 1:Distribution of responses on the preferred OAD therapy in T2DM
individuals newly diagnosed with HF
Figure 1:Distribution of responses on the preferred OAD therapy in T2DM
individuals newly diagnosed with HF
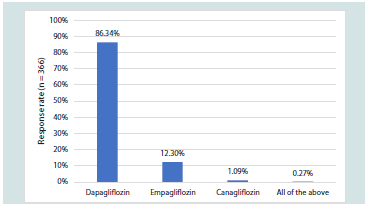 Figure 2:Distribution of responses on the most preferred SGLT2i for T2DM
individuals with established HF
Figure 2:Distribution of responses on the most preferred SGLT2i for T2DM
individuals with established HF
Research Article
Clinician Perspectives on Cardiovascular Risk–Based Use of DPP-4 and SGLT2 Inhibitors in Type 2 Diabetes Mellitus in Indian Settings
Manjula S* and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India.
*Address for Correspondence:Dr Manjula S, Department of Medical Services, Micro Labs
Limited, Bangalore, Karnataka. E-mail Id: drmanjulas@gmail.com
Submission: 16 April, 2026
Accepted: 06 May, 2026
Published: 08 May, 2026
Copyright: © 2026 Manjula S, et al. This is an open access
article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is
properly cited.
Keywords:Type 2 diabetes mellitus; Cardiovascular risk; Glycemic variability; DPP-4
inhibitors; SGLT2 inhibitors; Sitagliptin; Dapagliflozin
Abstract
Objective: The survey aimed to assess clinicians’ perspectives and preferences in
managing type 2 diabetes mellitus (T2DM), with particular emphasis on cardiovascular
risk–based decision-making and the use of dipeptidyl peptidase-4 (DPP-4) inhibitors
and sodium-glucose co-transporter-2 (SGLT2) inhibitors in routine clinical practice.
Methodology: This cross-sectional study was conducted among clinicians across
India to assess clinical perspectives in the management of T2DM with cardiovascular
risk, heart failure (HF), and chronic kidney disease (CKD). A structured 22-item,
multiple-response questionnaire was distributed via digital platforms, and responses
were analyzed using descriptive statistics to summarize clinician preferences and
experiences.
Results: A total of 366 clinicians participated in the survey. Nearly 34% of clinicians identified the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin as their preferred initiation therapy for newly diagnosed individuals with T2DM and cardiovascular risk. Approximately 80% of respondents reported sitagliptin as their preferred DPP-4 inhibitor. Around 70% of clinicians favored switching to a triple combination of metformin, a DPP-4 inhibitor, and an SGLT2 inhibitor in patients inadequately controlled on sulphonylurea plus metformin therapy. Among newly diagnosed individuals with T2DM and HF, 49% preferred the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin as the oral antidiabetic regimen. Nearly 86% of participants favored dapagliflozin as the preferred SGLT2 inhibitor in patients with established HF.
Conclusion: This survey indicates that clinicians frequently encounter individuals with T2DM presenting with cardiovascular risk. Physicians predominantly favor combination regimens incorporating DPP-4 inhibitors and SGLT2 inhibitors due to their perceived benefits in achieving glycemic targets, reducing glycemic variability, and providing cardiovascular and renal protection.
Results: A total of 366 clinicians participated in the survey. Nearly 34% of clinicians identified the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin as their preferred initiation therapy for newly diagnosed individuals with T2DM and cardiovascular risk. Approximately 80% of respondents reported sitagliptin as their preferred DPP-4 inhibitor. Around 70% of clinicians favored switching to a triple combination of metformin, a DPP-4 inhibitor, and an SGLT2 inhibitor in patients inadequately controlled on sulphonylurea plus metformin therapy. Among newly diagnosed individuals with T2DM and HF, 49% preferred the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin as the oral antidiabetic regimen. Nearly 86% of participants favored dapagliflozin as the preferred SGLT2 inhibitor in patients with established HF.
Conclusion: This survey indicates that clinicians frequently encounter individuals with T2DM presenting with cardiovascular risk. Physicians predominantly favor combination regimens incorporating DPP-4 inhibitors and SGLT2 inhibitors due to their perceived benefits in achieving glycemic targets, reducing glycemic variability, and providing cardiovascular and renal protection.
Introduction
Approximately 589 million adults (1 in 9) are currently living
with diabetes globally, a figure with a rapidly increasing global
prevalence, projected to rise to 853 million by 2050. Type 2 diabetes
mellitus (T2DM) accounts for nearly 90-95% of all diabetes cases
and disproportionately affects low- and middle-income countries,
where approximately 81% of individuals with diabetes reside.[1] In
2024, India, one of the most affected countries, has an estimated adult
population of 947.3 million, with a diabetes prevalence of 10.5%,
accounting for approximately 89.8 million adults living with diabetes.
[2]
In addition to chronic hyperglycemia, T2DM is characterized by substantial microvascular and macrovascular complications, with cardiovascular disease representing the leading cause of morbidity and mortality. Among individuals with diabetes, cardiovascular disease accounts for approximately 80% of all mortality and 75% of all hospitalizations.[3] Patients with T2DM have a two- to four-fold increased risk of atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), and diabetic kidney disease (DKD), emphasizing the need for comprehensive cardiometabolic risk management.[4]
In addition to chronic hyperglycemia, T2DM is characterized by substantial microvascular and macrovascular complications, with cardiovascular disease representing the leading cause of morbidity and mortality. Among individuals with diabetes, cardiovascular disease accounts for approximately 80% of all mortality and 75% of all hospitalizations.[3] Patients with T2DM have a two- to four-fold increased risk of atherosclerotic cardiovascular disease (ASCVD), heart failure (HF), and diabetic kidney disease (DKD), emphasizing the need for comprehensive cardiometabolic risk management.[4]
In recent years, large cardiovascular outcome trials have reshaped
treatment strategies in T2DM.
Sodium-glucose co-transporter-2
(SGLT2) inhibitors have demonstrated significant reductions in
hospitalization for HF and favorable renal outcomes, while dipeptidyl
peptidase-4 (DPP-4) inhibitors continue to be widely used for their
glycemic efficacy, low risk of hypoglycemia, and weight neutrality.[5]
These developments have influenced clinical guidelines, which now
recommend tailoring therapy based on the presence of cardiovascular
disease, HF, and renal impairment.[6-8]
SGLT2 inhibitors represent a unique class of glucose-lowering
therapies that reduce plasma glucose through an insulin-independent
mechanism by inhibiting renal glucose reabsorption at the proximal
tubule (S1 segment), thereby promoting glucosuria. Beyond glycemic
control, they exert multisystem benefits including osmotic diuresis,
natriuresis, reduction in preload and afterload, improvement in
lowering of blood pressure, and weight reduction. These effects
have been associated with significant reductions in hospitalization
for HF and delayed progression of kidney disease, and the class is
increasingly recognized for its role in preventing and treating HF, with
or without T2DM.[9,10] DPP-4 inhibitors are antihyperglycemic
agents that enhance endogenous incretin activity by preventing
degradation of glucagon-like peptide-1 (GLP-1), thereby improving
glucose-dependent insulin secretion and suppressing glucagon
release. Although major cardiovascular outcome trials have largely
demonstrated cardiovascular neutrality for this class, DPP-4
inhibitors are widely used due to their favorable safety profile, low
risk of hypoglycemia, weight neutrality, and suitability across a broad
spectrum of patients. [11,12]
Current clinical guidelines now emphasize individualized
treatment strategies based not only on glycemic status but also on
the presence of ASCVD, HF, and chronic kidney disease. In this
context, drug class selection and molecule preference are increasingly
influenced by cardiovascular comorbidities and safety profiles.13
Understanding clinicians' preferences and practices in patients with
cardiovascular risk is important to characterize current treatment
patterns and inform clinical practice. Therefore, the present study
aims to assess clinicians' preferences in managing T2DM, particularly
in the context of cardiovascular risk and HF, with emphasis on DPP-4
inhibitors and SGLT2 inhibitors.
Methodology
A cross-sectional study was carried out among clinicians
specialized in managing T2DM in the major Indian cities from June
2025 to December 2025.
Questionnaire:
The questionnaire booklet titled SYMPHONY (Sitagliptin
and combinations in Type 2 Diabetes Management: Expert
Perspectives on efficacy and tolerability) study was sent to the doctors
(cardiologists, diabetologists, general physicians, and consulting
physicians) who were interested in participating in the study. A 23-
item structured, multiple-response questionnaire aimed to assess
clinicians' preferences, cardiovascular risk–based treatment strategies,
and the use of DPP-4 inhibitors and SGLT2 inhibitors in routine
clinical practice. The study was performed after obtaining approval
from Bangalore Ethics, an Independent Ethics Committee (ECR/355/
Indt/KA/2022), which was recognized by the Indian Regulatory
Authority, the Drug Controller General of India.
Participants:
A convenient sampling technique was used, and an invitation
was sent to professionals across India based on their expertise
and experience in treating T2DM in the month of March 2025 for
participation in this Indian survey. About 366 clinicians from major
cities of all Indian states, representing the geographical distribution,
shared their willingness to participate and provide necessary
data. Clinicians were instructed to complete the questionnaire
independently without consulting colleagues. Written informed
consent was obtained from each participant before the study began.
Statistical analysis:
The data were analyzed using descriptive statistics. Categorical
variables were presented as percentages to clearly illustrate their
distribution. As an exploratory perception-based survey, the analysis
was limited to descriptive statistics. The frequency of occurrence
and corresponding percentages were employed to represent the
distribution of each variable. Graphs were created to visualize the
distribution of the categorical variables, using Microsoft Excel (version
16.0.18025.20030).
Results
The study included 366 clinicians, of whom 57% stated that 21-
40% of patients with T2DM have more than one comorbidity, such
as ASCVD, HF, and DKD. Approximately 61% of clinicians reported
that 21–40% of newly diagnosed individuals with T2DM are at
cardiovascular risk. Around 44% of respondents indicated that the
most common cardiovascular risk factors observed among newly
diagnosed individuals with T2DM are older age (>45 years in males
and >55 years in females), a history of hypertension, and smoking
or tobacco use. Nearly half of the respondents (50.55%) reported
that male individuals have major ASCVD risk factors, whereas 44%
indicated that both males and females have an equal risk of major
ASCVD factors. More than half of the clinicians (51.91%) reported
that high glycemic variability is often observed in patients with T2DM
and ASCVD, while 43% indicated that it is observed sometimes.
The majority of respondents (82.24%) opined that high glycemic variability increases the risk of composite major adverse cardiovascular events (MACE), atrial fibrillation (AF), non-infarctrelated artery (non-IRA) revascularization, and end-stage kidney disease (ESKD) in individuals with T2DM. Approximately 34% of the clinicians reported that the preferred initiation therapy in newly diagnosed T2DM individuals with cardiovascular risk is DPP4i + SGLT2i + metformin [Table 1].
According to 48% of respondents, approximately 41–60% of patients achieve the HbA1c target of 7% within 3 months after the addition of dapagliflozin. A reduction in cardiovascular mortality was reported by 54% of respondents as the most prominent extraglycemic benefit following the addition of SGLT2 inhibitors in patients with T2DM and HF. More than half of the respondents (51.37%) agreed that dapagliflozin reduces the risk of atrial fibrillation in individuals with T2DM, irrespective of HF status. As reported by 42% of clinicians, the primary beneficial effect observed with the combination of a DPP-4 inhibitor and an SGLT2 inhibitor in individuals with T2DM is a low risk of hypoglycemia. Additionally, 41% of respondents reported observing multiple benefits with this combination therapy, including reduced glycemic variability, modest weight loss, favourable renal effects, moderate reductions in systolic blood pressure, and the convenience of once-daily dosing.
The majority of respondents (52.46%) reported that a lower risk of hypoglycemia is the primary reason for preferring DPP-4 inhibitors over sulfonylureas in elderly patients with T2DM and established cardiovascular disease (eCVD). Approximately 66% agreed that the addition of a DPP-4 inhibitor to SGLT2 inhibitor therapy decreases the frequency of genitourinary infections in patients with T2DM. As reported by 45% of clinicians, approximately 11-20% of patients use the newer single-pill combination of sitagliptin, glimepiride, and metformin. A significant proportion of respondents (83.61%) reported that they have not observed any adverse drug reactions in patients treated with sitagliptin. Regarding glycemic control with sitagliptin, 42.9% of respondents reported marked improvement, while 41% reported moderate improvement.
The majority of respondents (82.24%) opined that high glycemic variability increases the risk of composite major adverse cardiovascular events (MACE), atrial fibrillation (AF), non-infarctrelated artery (non-IRA) revascularization, and end-stage kidney disease (ESKD) in individuals with T2DM. Approximately 34% of the clinicians reported that the preferred initiation therapy in newly diagnosed T2DM individuals with cardiovascular risk is DPP4i + SGLT2i + metformin [Table 1].
According to 48% of respondents, approximately 41–60% of patients achieve the HbA1c target of 7% within 3 months after the addition of dapagliflozin. A reduction in cardiovascular mortality was reported by 54% of respondents as the most prominent extraglycemic benefit following the addition of SGLT2 inhibitors in patients with T2DM and HF. More than half of the respondents (51.37%) agreed that dapagliflozin reduces the risk of atrial fibrillation in individuals with T2DM, irrespective of HF status. As reported by 42% of clinicians, the primary beneficial effect observed with the combination of a DPP-4 inhibitor and an SGLT2 inhibitor in individuals with T2DM is a low risk of hypoglycemia. Additionally, 41% of respondents reported observing multiple benefits with this combination therapy, including reduced glycemic variability, modest weight loss, favourable renal effects, moderate reductions in systolic blood pressure, and the convenience of once-daily dosing.
The majority of respondents (52.46%) reported that a lower risk of hypoglycemia is the primary reason for preferring DPP-4 inhibitors over sulfonylureas in elderly patients with T2DM and established cardiovascular disease (eCVD). Approximately 66% agreed that the addition of a DPP-4 inhibitor to SGLT2 inhibitor therapy decreases the frequency of genitourinary infections in patients with T2DM. As reported by 45% of clinicians, approximately 11-20% of patients use the newer single-pill combination of sitagliptin, glimepiride, and metformin. A significant proportion of respondents (83.61%) reported that they have not observed any adverse drug reactions in patients treated with sitagliptin. Regarding glycemic control with sitagliptin, 42.9% of respondents reported marked improvement, while 41% reported moderate improvement.
A significant proportion (79.78%) reported that sitagliptin
is the preferred DPP-4 inhibitor for individuals with T2DM and
cardiovascular risk (Table 2). Approximately 43% of participants
indicated that established cardiovascular outcome trial (CVOT)
evidence and demonstrated cardiovascular benefits, along with good
tolerability in patients with nonalcoholic fatty liver disease (NAFLD),
a lower risk of hypoglycemia, weight neutrality, and suitability across
different stages of T2DM, are key factors influencing their decision to
prefer sitagliptin in individuals with cardiovascular risk.
As reported by 58% of the experts, approximately 30–50% of patients with T2DM are inadequately controlled on sulphonylurea plus metformin therapy. More than half of the participants (69.67%) reported that switching to a triple combination of metformin, a DPP-4 inhibitor, and an SGLT2 inhibitor is the preferred add-on strategy for managing patients with T2DM who are uncontrolled on sulphonylurea plus metformin therapy (Table 3).
As indicated by 49% of clinicians, the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin is the preferred oral antidiabetic drug (OAD) therapy for individuals with T2DM newly diagnosed with HF [Figure 1]. The majority of clinicians (86.34%) reported that dapagliflozin is the preferred SGLT2 inhibitor for individuals with T2DM and established HF [Figure 2].
As reported by 58% of the experts, approximately 30–50% of patients with T2DM are inadequately controlled on sulphonylurea plus metformin therapy. More than half of the participants (69.67%) reported that switching to a triple combination of metformin, a DPP-4 inhibitor, and an SGLT2 inhibitor is the preferred add-on strategy for managing patients with T2DM who are uncontrolled on sulphonylurea plus metformin therapy (Table 3).
As indicated by 49% of clinicians, the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin is the preferred oral antidiabetic drug (OAD) therapy for individuals with T2DM newly diagnosed with HF [Figure 1]. The majority of clinicians (86.34%) reported that dapagliflozin is the preferred SGLT2 inhibitor for individuals with T2DM and established HF [Figure 2].
Discussion
The study highlights current cardiovascular-focused treatment
practices for T2DM in Indian clinical settings, with particular
emphasis on the use of DPP-4 inhibitors and SGLT2 inhibitors. In the
present study, the majority of participants reported that the preferred
initiation therapy in newly diagnosed individuals with T2DM and
cardiovascular risk was the combination of a DPP-4 inhibitor, an
SGLT2 inhibitor, and metformin. This preference reflects a shift
toward early combination therapy aimed at achieving comprehensive
metabolic and cardiovascular risk management rather than glucosecentric
management alone.
These findings are consistent with previously published Indian data. Bafna et al. reported that 74% of clinicians strongly recommended the triple fixed-dose combination of an SGLT2 inhibitor (dapagliflozin) with a DPP-4 inhibitor (sitagliptin) and metformin for patients with T2DM and cardiovascular or renal risk. [14] A prior survey conducted by the current authors similarly highlighted that the majority of physicians prescribed sitagliptin and dapagliflozin (DPP-4 inhibitor + SGLT2 inhibitor) specifically for newly diagnosed individuals with T2DM and cardiovascular risk.[15] Furthermore, Sahay et al. concluded that the preferred initiation therapy in newly diagnosed individuals with T2DM and cardiovascular risk in India includes DPP-4 inhibitors and SGLT2 inhibitors, particularly in those inadequately controlled on metformin monotherapy.[16] Likewise, Das et al. demonstrated that for newly diagnosed individuals with T2DM and HbA1c >7.5%, the preferred initiation therapy was a combination of DPP-4 inhibitors and metformin, based on expert consensus among diabetes specialists.[17] A significant proportion of respondents in the current survey reported that sitagliptin is the most preferred DPP-4 inhibitor for individuals with T2DM and cardiovascular risk. Consistent with prior observational studies and expert consensus statements, sitagliptin appears to be widely favored because of its established efficacy, favorable cardiovascular safety profile, and overall tolerability across diverse patient populations.[18-20] Kumar et al. concluded that sitagliptin was the most preferred DPP-4 inhibitor for individuals with T2DM and cardiovascular risk in India.[18] Similarly, Kalra et al. reported that sitagliptin is a preferred DPP-4 inhibitor for T2DM management in India due to its efficacy and safety when used as monotherapy, in combination, or as an add-on therapy.[20]
These findings are consistent with previously published Indian data. Bafna et al. reported that 74% of clinicians strongly recommended the triple fixed-dose combination of an SGLT2 inhibitor (dapagliflozin) with a DPP-4 inhibitor (sitagliptin) and metformin for patients with T2DM and cardiovascular or renal risk. [14] A prior survey conducted by the current authors similarly highlighted that the majority of physicians prescribed sitagliptin and dapagliflozin (DPP-4 inhibitor + SGLT2 inhibitor) specifically for newly diagnosed individuals with T2DM and cardiovascular risk.[15] Furthermore, Sahay et al. concluded that the preferred initiation therapy in newly diagnosed individuals with T2DM and cardiovascular risk in India includes DPP-4 inhibitors and SGLT2 inhibitors, particularly in those inadequately controlled on metformin monotherapy.[16] Likewise, Das et al. demonstrated that for newly diagnosed individuals with T2DM and HbA1c >7.5%, the preferred initiation therapy was a combination of DPP-4 inhibitors and metformin, based on expert consensus among diabetes specialists.[17] A significant proportion of respondents in the current survey reported that sitagliptin is the most preferred DPP-4 inhibitor for individuals with T2DM and cardiovascular risk. Consistent with prior observational studies and expert consensus statements, sitagliptin appears to be widely favored because of its established efficacy, favorable cardiovascular safety profile, and overall tolerability across diverse patient populations.[18-20] Kumar et al. concluded that sitagliptin was the most preferred DPP-4 inhibitor for individuals with T2DM and cardiovascular risk in India.[18] Similarly, Kalra et al. reported that sitagliptin is a preferred DPP-4 inhibitor for T2DM management in India due to its efficacy and safety when used as monotherapy, in combination, or as an add-on therapy.[20]
The preference for triple combination therapy comprising
metformin, a DPP-4 inhibitor, and an SGLT2 inhibitor, as noted
in the present survey, reflects evolving cardiometabolic treatment
strategies in routine clinical practice. Clinical studies, and metaanalyses
have consistently demonstrated that this combination
provides superior glycemic control compared with dual therapy,
along with additional benefits such as reductions in body weight and
blood pressure, without compromising safety.[21-23] A recent phase
3 study by Singh et al. showed that a fixed-dose triple combination
of dapagliflozin, sitagliptin, and metformin is effective and well
tolerated, offering improved glycemic control compared with dual
therapy.[21] In addition, a meta-analysis by Li et al. reported that the
addition of an SGLT2 inhibitor to a DPP-4 inhibitor plus metformin
(triple therapy) resulted in significantly greater reductions in blood
glucose levels, body weight, and blood pressure compared with dual
therapy.[23]
The current study further demonstrated that the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin was the preferred oral antidiabetic therapy in newly diagnosed T2DM individuals with HF. This finding is clinically relevant, given the established cardiovascular and HF benefits associated with SGLT2 inhibitors and the neutral cardiovascular safety profile of DPP-4 inhibitors. Supporting this observation, Chadha et al. reported that the combination of a DPP-4 inhibitor and an SGLT2 inhibitor is particularly beneficial for individuals with T2DM due to its favorable effects on glycemic parameters and vascular risk.[24] The present survey results identified dapagliflozin as the preferred SGLT2 inhibitor for individuals with T2DM and established HF. This preference is consistent with the expanding body of evidence supporting its cardiovascular and renal benefits beyond glycemic control. Ghosh et al. reported that dapagliflozin is commonly preferred in Indian clinical practice for patients with T2DM and established HF because of its synergistic effects on glycemic improvement and cardio-renal protection.[25] Similarly, Shaline Rao highlighted that dapagliflozin is a preferred SGLT2 inhibitor for the treatment of HF in patients with and without T2DM, noting that it was the first agent in its class to receive US FDA approval for this indication.[26] Mehta et al. further observed that, among available SGLT2 inhibitors, dapagliflozin was the most frequently preferred option in routine practice, particularly for cardiovascular and renal risk reduction in patients with T2DM.[27] These findings support the prominent role of dapagliflozin in cardiometabolic risk management.
The current study further demonstrated that the combination of a DPP-4 inhibitor, an SGLT2 inhibitor, and metformin was the preferred oral antidiabetic therapy in newly diagnosed T2DM individuals with HF. This finding is clinically relevant, given the established cardiovascular and HF benefits associated with SGLT2 inhibitors and the neutral cardiovascular safety profile of DPP-4 inhibitors. Supporting this observation, Chadha et al. reported that the combination of a DPP-4 inhibitor and an SGLT2 inhibitor is particularly beneficial for individuals with T2DM due to its favorable effects on glycemic parameters and vascular risk.[24] The present survey results identified dapagliflozin as the preferred SGLT2 inhibitor for individuals with T2DM and established HF. This preference is consistent with the expanding body of evidence supporting its cardiovascular and renal benefits beyond glycemic control. Ghosh et al. reported that dapagliflozin is commonly preferred in Indian clinical practice for patients with T2DM and established HF because of its synergistic effects on glycemic improvement and cardio-renal protection.[25] Similarly, Shaline Rao highlighted that dapagliflozin is a preferred SGLT2 inhibitor for the treatment of HF in patients with and without T2DM, noting that it was the first agent in its class to receive US FDA approval for this indication.[26] Mehta et al. further observed that, among available SGLT2 inhibitors, dapagliflozin was the most frequently preferred option in routine practice, particularly for cardiovascular and renal risk reduction in patients with T2DM.[27] These findings support the prominent role of dapagliflozin in cardiometabolic risk management.
In addition to therapeutic preferences, the current survey also
provided insights into tolerability patterns. A substantial proportion
of respondents (83.61%) reported not observing any adverse drug
reactions in patients treated with sitagliptin. This observation aligns
with previously published regional data. Sudhakaran et al. concluded
that sitagliptin effectively reduced glycemic parameters in individuals
with T2DM and was associated with a low incidence of adverse
experiences.[28] Mohan et al. similarly reported that sitagliptin was
generally well tolerated in Chinese, Indian, and Korean patients with
T2DM, with a low incidence of serious adverse events; most reported
events were mild and self-limiting.[29]
This nationwide cross-sectional survey involving 366 clinicians provides valuable insights into contemporary cardiovascular-focused management of T2DM in India, particularly regarding the use of DPP-4 inhibitors and SGLT2 inhibitors. Its strengths include a relatively large and geographically diverse sample, a comprehensive 23-item structured questionnaire capturing initiation strategies, add-on therapy, drug selection rationale, and safety perceptions, and a clear descriptive statistical presentation of findings. The focus on cardiometabolic risk, including ASCVD, HF, and DKD, enhances its clinical relevance in the context of evolving guideline-directed care. However, the study has limitations inherent to survey-based research, including its cross-sectional design, reliance on self-reported physician perceptions rather than audited prescription or patient-level outcome data, potential recall and response bias, and the use of descriptive statistics without inferential analysis. Furthermore, the survey did not include patient-level clinical data, treatment adherence information, or longitudinal cardiovascular and renal outcomes. Therefore, while the findings provide insight into prevailing therapeutic preferences, they do not establish the clinical effectiveness or safety of the reported strategies in the patient population. These limitations should be considered when interpreting the results, and future prospective studies incorporating prescription audits and outcome-based clinical data would help validate and expand upon these observations.
This nationwide cross-sectional survey involving 366 clinicians provides valuable insights into contemporary cardiovascular-focused management of T2DM in India, particularly regarding the use of DPP-4 inhibitors and SGLT2 inhibitors. Its strengths include a relatively large and geographically diverse sample, a comprehensive 23-item structured questionnaire capturing initiation strategies, add-on therapy, drug selection rationale, and safety perceptions, and a clear descriptive statistical presentation of findings. The focus on cardiometabolic risk, including ASCVD, HF, and DKD, enhances its clinical relevance in the context of evolving guideline-directed care. However, the study has limitations inherent to survey-based research, including its cross-sectional design, reliance on self-reported physician perceptions rather than audited prescription or patient-level outcome data, potential recall and response bias, and the use of descriptive statistics without inferential analysis. Furthermore, the survey did not include patient-level clinical data, treatment adherence information, or longitudinal cardiovascular and renal outcomes. Therefore, while the findings provide insight into prevailing therapeutic preferences, they do not establish the clinical effectiveness or safety of the reported strategies in the patient population. These limitations should be considered when interpreting the results, and future prospective studies incorporating prescription audits and outcome-based clinical data would help validate and expand upon these observations.
Conclusion
This survey indicates a clear preference among clinicians for early
combination therapy incorporating DPP-4 inhibitors and SGLT2
inhibitors, particularly sitagliptin- and dapagliflozin-based regimens,
in individuals with cardiovascular risk and heart failure. The strong
inclination toward triple therapy with metformin, a DPP-4 inhibitor,
and an SGLT2 inhibitor suggests a shift from glucose-centric
treatment toward comprehensive cardiometabolic risk reduction.
Sitagliptin was reported as the preferred DPP-4 inhibitor due to
its perceived efficacy, cardiovascular safety, and tolerability, while
dapagliflozin is favored for its established cardio-renal benefits and
heart failure outcomes.
Acknowledgement
We would like to thank all the clinicians who participated in this
study.
Conflict of interest:
Both authors are employees of Micro Labs Limited. The study was
designed and conducted as part of a scientific initiative. The authors
declare that no undue influence was exerted on data collection,
analysis, or interpretation.
Funding:
This study was funded by Micro Labs Limited. The sponsor had
a role in study conceptualization and questionnaire development but
did not influence the interpretation of results.
References
Citation
Manjula S, Krishna Kumar M. Clinician Perspectives on Cardiovascular Risk–Based Use of DPP-4 and SGLT2 Inhibitors in Type 2 Diabetes Mellitus in Indian Settings. Adv Diabetes Endocrinol 2026;9(1): 1.