
Case Report
Follicular Thyroid Cancer: An Unusual Metastasis to the Right Atrium Case Report and Literature Review
Osman A Hamour* and Sarah Sahel
- King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia
*Address for Correspondence: Osman A Hamour, King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia; E-mail: osmanahamour@gmail.com
Citation: Hamour OA, Sahel S. Follicular Thyroid Cancer: An Unusual Metastasis to the Right Atrium Case Report and Literature Review. Adv Diabetes Endocrinol 2017;2(1): 3.
Copyright: © 2017 Hamour OA, et al. This is an open access articledistributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Advances in Diabetes & Endocrinology | ISSN: 2475-5591 | Volume: 2, Issue: 1
Submission: 20 February, 2017| Accepted: 04 April, 2017 | Published: 11 April, 2017
Abstract
Background: Follicular Thyroid Cancer (FTC) is one type of the group of Differentiated Thyroid Cancer (DTC). It constitutes about 10% of this group. DTC is a rare disease and it remains to have a favorable prognosis in comparison to other forms of malignancy, with diseasespecific death rates as low as 1.3%. FTC has different biological characteristics, so unlike the more common Papillary Type (PTC), FTC has the ability for haematogenous spread.
Case review: A 54-year-old woman presented with a thyroid swelling (FTC) causing progressive respiratory obstructive symptom. The swelling was clinically huge with retrosternal extension. Computed Tomography (CT) revealed destruction of medial part of the clavicle and sternum. It also showed encasement of the major neck vessels with extension in the right atrium.
Methods: After an Institutional Review Board approval was granted (IRB) information about the case was collected by direct interview and by medical file review.
Conclusion: FTC can present in an aggressive form and spread widely to destroy bones and encase major vessels including the heart as in this case. Though the standard treatment of DTC is surgical, in some cases any surgery other than taking a generous biopsy might be hazardous and pre-operative radiotherapy might be the only viable option.
Keywords
FTC; Local bone destruction; Major vessels encasement; Right atrium
Introduction
FTC is the second most common thyroid cancer after papillary thyroid cancer. Its prognosis depend on many factors mainly the age and the pathological staging [1,2]. Other factors include distant metastasis, vascular and capsular invasion, tumor size, early recurrence, hurthle cell carcinoma type and insular cancer [1,3-5].
Up to 25% of FTC has distant metastasis [6]. It typically spreads via haematogenous metastasis, thus, spread to lymph node is uncommon. Common distant metastasis are bone and lung and, less commonly, liver, brain, bladder and, skin.
The mainstay of treatment is surgical removal of the tumor with total or near-total thyroidectomy. Followed by radioactive iodine therapy, then life-long thyroid hormone replacement. External Beam Radiation Therapy (EBRT) is used in some situations, like, older patients with non respectable tumor, or those resistant to RAI, or in patient with spinal cord compression or painful bony lesion.
In this case report, the presentation is uniquely different. The initial presentation has already included bone metastasis, encasement of major blood vessels and involvement of the right atrium. The large size tumor as well as the extensive spread to adjacent bony structures, and the right atrium involvement make surgical resection heroic and unfeasible if not impossible.
Case Report
A 54-year-old woman presented to the surgical clinic with a long standing history of a neck mass occupying the anterior part of her neck. The swelling moves with swallowing. The mass was gradually increasing in size until eventually it started to cause obstructive symptoms in the form of shortness of breath on minor exertion, difficulty in swallowing, snoring and very troublesome sleep apnea. There was no history of change of voice, or weight loss. The systemic review was normal. She was not diabetic, but known hypertensive on treatment. There was no family history of thyroid or other endocrine disease. She was not a smoker and she does not drink alcohol. On examination she was a pleasant morbidly obese lady with a BMI of 36. There was a big mass in the anterior part of the neck arising from the thyroid gland, involving mainly the right lobe with retrosternal extension. There were no signs of hypothyroidism or hyperthyroidism. The other systems examination was normal.
Her full blood count, renal profile, and liver profile were all normal. Thyroglobulin level was over 5000 units and the thyroglobulin antibodies was 501 units. Ultrasound scan of the neck and an ultrasound guided FNA were done as shown in (Figure 1). Ultrasound scan of the neck showed a large right thyroid mass with eggshell calcification extending to the midline. The right thyroid lobe was enlarged at 6.2 X 5.9 X 3.9 cm and the left thyroid lobe was 2.9 X 5 X 2.8 cm. benign looking lymph nodes were seen bilaterally.
A Fine Needle Aspiration biopsy [FNAB] was taken from the right thyroid lobe showed cells suspicious of follicular neoplasm. Considering the clinical picture, an open biopsy under local anesthesia was taken from the same site. It showed a well differentiated follicular thyroid carcinoma which was positive for vascular invasion. At this stage a CT scan of the chest and neck was done to stage the tumor (Figure 2 and 3).
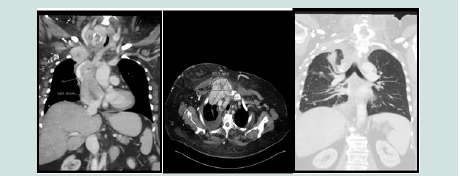

CT Chest showed a destructive soft tissue mass extending into the sternum, right first rib, and possible extension to the right clavicle (Figure 2 a-c). There was a large filling defect in the right atrium extending to the superior vena cava.
CT neck showed a partially encased right common carotid artery by the tumor at the level of superior mediastinum and thoracic inlet with no definitive clear line between it and the tumor (Figure 3 a,b). The right internal jugular vein was displaced laterally and inseparable from the adjacent lesion starting from the level of the right subclavian confluence for about 4 cm cranially. The huge right thyroid mass lesion showed huge soft tissue mass effect on the adjacent airway.
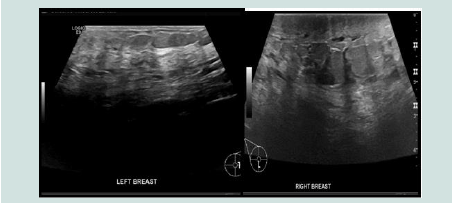
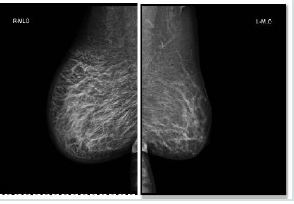
CT abdomen showed no intra-abdominal metastasis. The patient’s case was discussed in the Multi-Disciplinary-Team (MDT) meeting and the recommendations was that the disease is too advanced to be removed surgically and the patient is to go for external beam radiation therapy and to be assessed after the therapy is completed. The patient showed remarkable clinical improvement after the radiotherapy especially from the airway side, all the respiratory symptoms improved as well as the sleep apnea and the choking sensation. Cardio thoracic team assessed the patient and their verdict that surgical intervention from their side is not possible due to the advanced disease she had. Patient was well informed and was kept under close surveillance until she presented one day with pain and diffuse skin thickening of her right breast, which was attributed to the radiotherapy she had, and was advised to do an ultrasound and mammogram (Figure 4), which were both reported to show thickened skin with tissue edema on the right breast most likely due to metastasis from the FTC. But no definitive lesion, no biopsy was obtained. The left breast was normal there was only one benign-looking lymph node in the left axilla.
Patient was not satisfied with her treatment plan and she preferred to go for a second opinion outside the country. As prophylactic measures, patient was started on Aspirin. Later on in the course of her disease, she developed progressive shortness of breath, so CT chest and neck was repeated. It showed progressive and advance involvement of the major blood vessels, with new finding of multiple bilateral lung metastases and large pleural effusion on the right side. US guidance drainage was done and fluid was sent for biochemical testing, microbiology, and cytology. The cytology was negative for malignant cells and the fluid biochemical testing results were all normal except for elevated RBC of 343. Fluid culture was also negative for any growth.
Discussion
This is a case of advance follicular thyroid cancer with unusual presentation. The disease is typically spreads via haematogenous dissemination and the metastasis occur in 10 to 15% of patients. The common sites of metastasis are bone (with lytic lesion) and lung and, less commonly, the brain, liver, bladder and skin. In this case, she had atypical pattern of distant metastasis-although she had metastasis to the bone and lung - in which it involved major vessels and cardiac structure i.e., right atrium. There’s only few similar cases reported worldwide that had right atrium and major vessels involvement. Namely 3 cases were reported with heart metastasis but at different sites (2 were in the right ventricles and 1 in the pericardium). All cases have no involvement of the great vessels. In all 3 cases, total thyroidectomy was performed, followed by radioactive iodine. The outcome appeared to have good result. Which we couldn’t achieve in this case due to radiological evidence of encasement and involvement of right IJV, right carotid, SVC and right atrium.
Conclusion
This is an unusual case of follicular thyroid cancer with initial presentation of a neck mass with distant metastasis to the right atrium and SVC. Surgical resection was too dangerous to be performed due to extensive involvement of the cardiovascular vital structures. Unfortunately, palliative treatment was the only option available for us.
References
- Grebe SK, Hay ID (1995) Follicular thyroid cancer. Endocrinol Metab Clin North Am 24: 761-801.
- Mazzaferri EL, Jhiang SM (1994) Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 97: 418-428.
- Lin JD, Hsueh C, Chao TC (2009) Early recurrence of papillary and follicular thyroid carcinoma predicts a worse outcome. Thyroid 19: 1053-1059.
- Kushchayeva Y, Duh QY, Kebebew E, D’Avanzo A, Clark OH (2008) Comparison of clinical characteristics at diagnosis and during follow-up in 118 patients with hurthle cell or follicular thyroid cancer. Am J Surg 195: 457-462.
- Lai HW, Lee CH, Chen JY, Tseng LM, Yang AH (2006) Insular thyroidcarcinoma: collective analysis of clinicohistologic prognostic factors and treatment effect with radioiodine or radiation therapy. J Am Coll Surg 203: 715-722.
- Mazzaferri EL (1993) Thyroid carcinoma, papillary and follicular. In: Mazzaferri EL, Samaan NA (Eds), Endocrine Tumors. Blackwell Scientific, Cambridge, MA. pp. 278.