
Journal of Surgery
Download PDF
Research Article
*Address for Correspondence: Zhang Zhe, Department of Thoracic Surgery, Qingdao Municipal Hospital, Qingdao 266011, Shandong Province, China, E-mail: doctorzhangzhe@aliyun.com
Citation: Xing-long F, Di Z, Lu Z, Yu-xia L, Hong-xian C, Zhe Z. Trans Oral-Substernum Incision Thoracic Endoscopic Surgery: A Minimally Invasive Endoscopic Approach in Thoracic Surgery. J Surgery. 2015;3(2): 3.
Copyright © 2015 Xing-long F, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 3, Issue: 2
Submission: 06 August 2015 | Accepted: 09 September 2015 | Published: 14 September 2015
Reviewed & Approved by: Dr. Filipe Moreira de Andrade, Professor of Pulmonology & Thoracic Surgery, Universidade Federal de Viçosa, Brazil
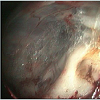
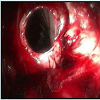
When the tunnel reached the strenal incisure, a grasping forceps was inserted through another working tunnel to assist the separation. In this site care had to be taken not to injure the left brachiocephalic veins. The fascia was be dissected by scissors clung to sternum. When fascia was cut off, the space under sternum (Anterior mediastinum) appeared (figure 2). Video gastroscope was then introduced through the port to replace the Needlescopy, and a total anterior mediastinal exploration was performed. With the use of CO2, a working place was made in the anterior mediastinum. The next step was the creation of mediastinal pleural windows. On the right side, a digital dissection of the right mediastinal pleura above the level of the superior vena cava was performed, creating a communication between the mediastinum and the right pleural cavity (figure 3). On the left side, the pleurotomy was also digitally performed over the ascending aorta. Video gastroscope was then introduced into the pleural cavities through both pleurotomies.
Trans Oral-Substernum Incision Thoracic Endoscopic Surgery: A Minimally Invasive Endoscopic Approach in Thoracic Surgery
Fan Xing-long2, Zahng Di1, Zhang Lu1, Liu Yu-xia1, Cui Hong-xian1 and Zhang Zhe1*
- 1Department of Thoracic Surgery, Qingdao Municipal Hospital, Qingdao 266011, Shandong Province, China
- 2Department of Thoracic Surgery, Qilu Hospital of Shandong University, Qingdao 266071, Shandong Province, China
*Address for Correspondence: Zhang Zhe, Department of Thoracic Surgery, Qingdao Municipal Hospital, Qingdao 266011, Shandong Province, China, E-mail: doctorzhangzhe@aliyun.com
Citation: Xing-long F, Di Z, Lu Z, Yu-xia L, Hong-xian C, Zhe Z. Trans Oral-Substernum Incision Thoracic Endoscopic Surgery: A Minimally Invasive Endoscopic Approach in Thoracic Surgery. J Surgery. 2015;3(2): 3.
Copyright © 2015 Xing-long F, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 3, Issue: 2
Submission: 06 August 2015 | Accepted: 09 September 2015 | Published: 14 September 2015
Reviewed & Approved by: Dr. Filipe Moreira de Andrade, Professor of Pulmonology & Thoracic Surgery, Universidade Federal de Viçosa, Brazil
Abstract
Flexible endoscope is used in Natural Orifice Trans-luminal Endoscopic Surgery. Cervical incision thoracic surgery has recently been described. The use of a flexible endoscope through a natural orifice into the thoracic cavity still remains ethically doubtful. The authors present a surgical experimental study using a flexible endoscope through oral-substernum incision for the exploration of both the thoracic cavity in dog model. An experimental work on 5 male mongrel dogs was initiated. Through a small incision at oral floor, we performed simultaneous exploration of the pleural cavities. Identification and biopsies of pleural and lung was performed. None chest tube was placed in the thoracic cavity at the end of all pleural procedures. The potential advantages of this approach are exploration of the thoracic cavity and the performance of several thoracic interventions through oral floor. The flexible endoscope could become a surgical tool for thoracic surgery.Keywords
Thoracoscopy; Endoscopic procedures; Minimally invasive surgery; Natural Orifice Trans-luminal Endoscopic Surgery (NOTES)Introduction
The treatment of lung cancer and other thoracic tumors usually involves thoracic surgeries. Cancer staging is a necessary step before cancer treatment. Mediastinal lymph nodes, pleural biopsies and lung biopsies are frequently needed for staging tumors. Despite the development of less invasive techniques, such as trans-bronchial needle aspiration (TBNA), endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA), and more recently, endobronchial ultrasoundguided fine-needle aspiration (EBUS-FNA), mediastinoscopy and video-thoracoscopy still remain the more satisfactory and commonly performed invasive techniques for mediastinal and pleural staging of thoracic tumors [1,2]. The development of thoracoscopic approaches during the early 1990s excited thoracic surgeons due to multiple advantages of this technique. Thoracoscopy unquestionably decreased the length of hospital stay, hospital cost, and rate of scar complications; and provided some cosmetic advantages. However, it did not significantly reduce postoperative pain. Thoracic ports and chest tubes are a major cause of persistent pain [3]. Minimally invasive techniques in thoracic surgery are evolving. And several recent thoracic surgical interventions were performed through cervical incisions [4,5]. There is a trend in favor of using flexible endoscopy in general surgery [6]. Flexible endoscope is used in Natural Orifice Trans-luminal Endoscopic Surgery (NOTES) techniques [7]; and few cases were reported on its application in abdominal surgery. Latest attempts in minimizing surgical trauma lead to an experimental trans oral access to the mediastinal for lymph node biopsies. Human application has been described for NOTES in thoracic surgery [8], but ethical restraints and the risk of major mediastinal complications limit its application on humans. The aim of this experimental work on animal is to evaluate the use of flexible endoscope for the exploration of thoracic cavity and pleura through a single trans oral incision.Materials and Methods
The experimental protocol of this study (No.KYLL-2014(KS)-12) was granted by the Institutional Ethic Committee of Qingdao Municipal Hospital. The study was conducted according to the Declaration of Helsinki. All animals received human care in compliance.Five male mongrel dogs were used to evaluate the feasibility and safety of the trans-oral endoscopic thoracic surgery through the floor of the mouth. Intravenous anesthesia was induced with ketamine, midazolam, and azaperone, and pancuronium as relxant. Due to the length of dog’s neck, intubation was performed by tracheotomy at the middle of trachea. The incision was sutured after intubation. Ventilation was controlled with standard ventilation system (Evita XL, Drager, Lubeck/Germany). We used Needlescopy (5.0 mm, 30°), standard double-channel flexible video gastroscope (Olypus), and endoscopic video Monitor. The trocar used Triport Laparoscopic Instrument Port.
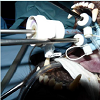
The dog was positioned in supine position on the operation table with reclination of the head. The mucosa in the vestibule of mouth was incised. A 10 mm sublingual sagittal incision was made between the papillae of the Wharton duct in the middle line. The mental nerve was taken care of. The muscles of the oral floor (geniohyoid muscle, mylohyoid muscle, and anterior belly of the digastric muscle) were separated directly in the midline by scissors. The separate direction pointed to neck subcutaneous. The incision was divided along the plane between the superficial fascia and the subcutaneous. When the work tunnel was made by sharp dissection along the middle of neck, the triport was inserted into the tunnel (figure 1). The working space was created with scissors under the vision of Needlescopy, which was inserted into the tunnel through the port. CO2 was insufflated into tunnel to create the working space at 4.0-6.0 mm Hg pressure. In this way, the working space was made easily with scissors under vision from oral floor to the sternal incisure. The jugular venous arch could be cut only when the space was made far from subcutaneous.
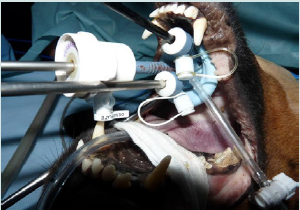
Figure 1: The triport was inserted into the tunnel.
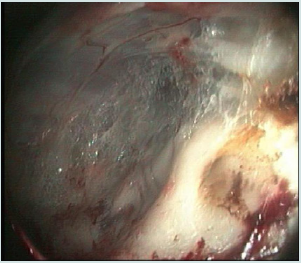
Figure 2: When fascia was cut off, the space under sternum (Anterior mediastinum) appeared.
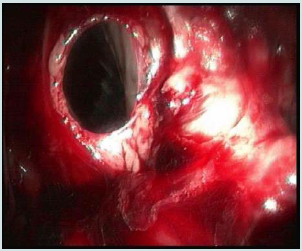
Figure 3: On the right side, a digital dissection of the right mediastinal pleura above the level of the superior vena cava was performed, creating a communication between the mediastinum and the right pleural cavity.
Results
The operative step was repeated in the experiments. In all experiments, no problems with operative procedure and anesthesia occurred. No major bleeding complication was noticed. With CO2 insufflated at 4.0-6.0 mm Hg pressure, the subcutaneous tissues got loosen as a result of the cutaneous emphysema. The working space was made easily with scissors under vision from oral floor to the sternal incisure.In all cases, the mediastinum was reached and the vascular structure could also be spared. Pleurotomy was digitally performed. Video gastroscope can be introduced into the pleural cavities through pleurotomies.
During the entire operative procedure, transcutanrous oxygen tension determination and venous blood gas analysis appeared normal, which indicated that the gas exchange and ventilation were not affected by CO2 at the pressure of 4.0-6.0 mm Hg pressure to the mediastinum.
The introduction of video gastroscope into the pleural cavities through the previously created mediastinal windows was not difficult; and it allowed a wide exploration of both pleural cavities. On all of the dogs, we performed bilateral pleural and lung biopsies using a grasp forceps. No chest tube was inserted into thoracic cavity after surgical procedure.
All dogs were breathing spontaneously after the operation. The tube could be extubated without difficulties. The dogs recovered quickly, and no acute bleeding occurred after the operation. The dogs were given food 6 hours after the operation. All animals started oral food intake without signs of pain. In the following 3 days, all dogs were fed with regular food and water. There were no signs of pain or local wound infections.
Discussion
The thoracoscopic approaches developed in the early 1990s disappointed thoracic surgeons. The persistence of postoperative pain remained an unresolved problem. The need for thoracic ports and chest tube are the major cause of this pain. Minimally invasive techniques in thoracic surgery have been evolving. Further development of sophisticated endoscopic instruments and increasing possibilities of camera and video technology over the last 5 years resulted in a paradigm shift: the use of nature orifices of human body as access route to endoscopic surgical procedure further minimized surgical trauma. This could be called the third generation surgery compared with the generation of visceral surgery (minimally invasive laparoscopic surgery in mid 1980s).NOTES mainly use flexible endoscopics or rigid endoscopics and instruments, and enter the body through natural orifices and cavities such as the stomach, the bladder, the vagina, or the esophagus. Most of the operations were performed with rigid endoscopics and instruments. The flexible endoscopics approaches are still under development. The major obstacle is that there are no appropriate flexible endoscopics or reliable endoscopic suturing technique.
The use of a flexible endoscope through a natural orifice (NOTES) into the thoracic cavity still remains ethically doubtful in humans as does the trans-oesophageal approach transgastric, or vaginal applications [9,10].
Jalal et al. described an approach in cervical incision thoracic endoscopic surgery (CITES), using a flexible endoscope though a validated cervical incision. The extreme flexibility of the endoscope offered the possibility of a complete pleural inspection, and it could be used for biopsies in several thoracic sites, and for the performance of more complicated surgical procedures (e.g. sympathectomy). Swantstrom et al. recently published a report on the use of flexible endoscope into the mediastinum through a cervical incision for Heller myotomy and oesophagectomy in six animals and one cadaver [11].
In the last 5 years, there have been several attempts to access the thorax. One way was from bladder to abdominal cavity and the diaphragm. Another path was transmural esophageal or hybrid approach via superasternal incision.
Recently, Wilhelm et al. presented their research that proved the safety and feasibility of the trans oral endoscopic approach for minimally invasive thyroidectomy [1-14]. They also published an important research on endoscopic approach for mediastinal surgery. In this way, trachea was easily identified and followed down to the mediastinum.
In our study, with standard laparoscopic instruments and CO2 insufflation, a sufficient working space was created. From oral floor along trachea through mediastinum, thoracic cavity and all natural structures intrathoracic was identified. Pleural and lung biopsy could also be performed by flexible endoscopics and instruments.
The advantage of this technique is the possibility of working in line with trachea and sternum. Only at the entrance of sternal incisure, the left brachiocephalic veins must be stretched. With the assistant of CO2 pressure, the working place can be made easily in the anterior mediastinum. The mediastinal pleural windows above the level of the superior vena cava and ascending aorta make the operation path safer than the other path. This technique can help avoid superior vena cava and left common carotid, and therefore the most important thing is that this operation path can avoid thorax infection caused by esophageal and trachea incision.
The limitation of the experiment was the subject. The neck of dog is longer than porcine. The double lumen endotracheal intubation must be performed after tracheotomy. The tracheotomy may bring detrimental influence to the study. The space between sternal incisure and the left brachiocephalic veins could be another problem.
In conclusion, this new trans-oral endoscopic approach for thoracic surgery was feasible in animal study. The dogs with short survival time showed the safety of the procedure. After a thorough preclinical study, our experience with minimally invasive thoracoscopy surgery indicates that benefits of trans-oral thoracoscopy can be expected.
Also when the patient was asked about the overall satisfaction regarding the incision used for OLT, a higher number of patients with J-shaped incision reported to be pleased than those with Mercedes type incision, 96% vs 75%. Although a fully subjective evaluation of the patient, this reflects attending physician impression. No adaptation in the retractor or surgical technique was necessary in order to gain full access to the liver for OLT.
Recently, Demirbas et al. reported a series of 32 patients submitted to living donor right hepatectomy using upper midline incision [15]. Use of this type of incision has not yet been reported in OLT.
Our results suggest that a J-shaped incision is preferred to other incisions for OLT.
There is a need for more detailed studies on the influence of the incision on the hepatectomy procedure, partial or total, because there are few reviews that explain about this.
References
- Detterbeck FC, Jantz MA, Wallace M, Vansteenkiste J, Silvestri GA, et al. (2007) Invasive mediastinal staging of lung cancer: ACCP evidence-based clinical practice guidelines, 2nd edition. Chest 132(3 Suppl): 202S-220S.
- Carlens E (1959) Mediastinoscopy: a method for inspection and tissue biopsy in the superior mediastinum. Dis Chest 36: 343-352.
- Rusch VW, Bains MS, Burt ME, McCormack PM, Ginsberg RJ (1994) Contribution of videothoracoscopy to the management of the cancer patient. Ann Surg Oncol 1: 94-98.
- Zielinski M, Pankowski J, Hauer L, Kuzdzal J, Nabialek T (2007) The right upper lobe pulmonary resection performed though the transcervical approach. Eur J Cardiothorac Surg 32: 766-769.
- Fowkes L, Lau KK, Shah N, Black E (2009) A cervical approach to investigating pleural disease. Ann Thorac Surg 88: 315-317.
- Swanstrom LL, Dunst CM, Spaun GO (2010) Future applications of flexible endoscopy in esophageal surgery. J Gastrointest Surg 14 Suppl 1: S127-S132.
- Perreta S, Dallemagne B, Coumaros D, Marescaux J (2008) Natural orifice transluminal endoscopic surgery: transgastric cholecystectomy in a survival porcine model. Surg Endosc 22: 1126-1130.
- Wilhelm T, Klemm W, Leschber G, Harlaar JJ, Kerver AL, et al. (2011) Development of a new trans-oral endoscopic approach for mediastinal surgery based on ‘natural orifice surgery’: preclinical studies on surgical technique, feasibility, and safety. Eur J Cardiothorac Surg 39: 1001-1008.
- Venissac N, Pop D, Mouroux J (2009) Video-assisted mediastinoscopy as a therapeutic tool. Surg Endosc 23: 2466-2472.
- Wilhelm T, Harlaar J, Kerver A, Kleinrensink GJ, Benhidjeb T (2010) Surgical anatomy of the floor of the oral cavity and the cervical spaces as a rationale for trans-oral, minimal-invasive endoscopic surgical procedures: results of anatomical studies. Eur Arch Otorhinolaryngol 267: 1285-1290.
- Wilhelm T, Benhidjeb T (2011) Transoral endoscopic neck surgery: feasibility and safety in a porcine model based on the example of thymectomy. Surg Endosc 25: 1741-1746.
- Call S, Rami-Porta R, Serra-Mitjans M, Saumench R, Bidegain C, et al. (2008) Extended cervical mediastinoscopy in the staging of bronchogenic carcinoma of the left lung. Eur J Cardiothorac Surg 34: 1081-1084.
- Benhidjeb T, Wilhelm T, Harlaar J, Kleinrensink GJ, Schneider TA, et al. (2009) Natural orifice surgery on thyroid gland: totally transoral video-assisted thyroidectomy (TOVAT): report of first experimental results of a new surgical method. Surg Endosc 23: 1119-1120.
- Wilhelm T, Metzig A (2010) Video. Endoscopic minimal-invasive thyroidectomy: first clinical experience. Surg Endosc 24: 1757-1758.