Journal of Pharmaceutics & Pharmacology
Download PDF
Research Article
Eribis Peptide 94 Mimics Ischemic Preconditioning in Rats with an Acute Myocardial Infarction and has Cardioprotective Effects during Prolonged Ischemia
Irina Bobrova1*, Oksana N. Khokhlova2, Elvira R.Shaykhutdinova2, Georgij Zoloev3, Herman Krapf1, Arkadij N. Murashev2 and Garrett J. Gross4
- 1Eribis Pharmaceuticals AB, Sweden
- 2Shemyakin and Ovchinnikov Institute of Bioorganic Chemistry RAS, Pushchino, Moscow Region, Russia
- 3Invalids Rehabilitation Center, Novokuznetsk, Russia
- 4Medical College of Wisconsin, USA
- Address for Correspondence: Irina Bobrova, Eribis Pharmaceuticals AB, Flisavagen 16, Vasteras, 72353, Sweden, Tel & Fax: +46-21-840415; E-mail: dynorph05@yahoo.se
Citation: Bobrova I, Khokhlova ON, Shaykhutdinova ER, Zoloev G, Krapf H, et al. Eribis Peptide 94 Mimics Ischemic Preconditioning in Rats with an Acute Myocardial Infarction and has Cardioprotective Effects during Prolonged Ischemia. J Pharmaceu Pharmacol. 2014;2(1): 6.
Copyright © 2014 Bobrova I, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pharmaceutics & Pharmacology | ISSN: 2327-204X | Volume: 2, Issue: 1
Submission: 08 April 2014 | Accepted: 13 May 2014 | Published: 19 May 2014
Reviewed & Approved by: Dr. Kunlin Jin, Professor, Department of Pharmacology and Neuroscience, University of North Texas Health Science Center, USAAbstract
Objectives: Previously, we demonstrated that a novel enkephalin analogue, Eribis Peptide 94 (EP94), produces a reduction of myocardial infarct size in rats and pigs administrated during occlusion. Since a complete dose-response relationship and the opioid receptor subtype activated by EP94 was not been clearly established, the following study was undertaken. It was also determined if multiple doses of EP94 could produce greater cardioprotective effects similar to those observed with single versus multiple ischemic preconditioning (IPC) stimuli.
Methods: We used adult male Sprague-Dawley rats subjected to either 25 or 40 minutes of coronary occlusion followed by 120 minutes of reperfusion.
Key findings: A single and triple bolus of 1 μg/kg of EP94 administered iv prior occlusion produced a reduction of infarct size (IS/AAR) by 39% and 45%, correspondingly. Dose-response relationship has been established. All of the opioid receptor antagonists (naloxone, CTOP, naltrindole, nor-BNI) blocked the effect of EP94.
Conclusion: EP94 produces a potent cardioprotective effect in rats following single or multiple injections administrated prior occlusion via effects on μ, δ, and κ opioid receptors. Repeated bolus injections of EP94 produced a reduction of IS/AAR when the ischemic period was increased from 25 to 40 minutes.Keywords
Cardioprotection; Enkephalin; Ischemia; Myocardial infarctionIntroduction
Involvement of opioid receptors and their endogenous ligands in the regulation of cardiac tolerance to ischemia/reperfusion supports an important role for enkephalins as a part of the endogenous opioid system responsible for cardioprotection. The development of cardioprotective agents, based on the enkephalin structure in order to improve myocardial function and limit the total extent of infarction during ischemia/reperfusion is of great clinical importance.Known synthetic enkephalin analogues (FK 33-824, Tyr-DAla-Gly-MePhe-Met(O)ol; DAMGO, DADLE, DPDPE, Dalargin, 2’,6’-dimethyltyrosine-D-Arg-Phe-Lys-NH2), native enkephalin sequences, (ME, LE, MEAP, proenkephalin), have been tested for involvement in cardioprotection in recent years. Some of them reduce myocardial ischemia/reperfusion injury when administered prior to, during or after the onset of ischemia [1,2]. However, few results have been obtained for therapeutic applications of potent cardioprotective opioids.As a part of our effort to obtain new enkephalin analogues [3-5] we have synthesized several new compounds with a cardioprotective profile [6] and tested them in a rat model of infarction.Eribis peptide 94 (EP94) is a tetrapeptidamide of the native enkephalin sequence with modifications in position 2 and 4. Full structural formula is presented in the patent description [6]. Novel enkephalin analog EP94 demonstrated high affinity for μ- and δ-opioid receptors. Studies of Gross et al. [7] suggest that EP94 injected during ischemia reduced infarct size in rat hearts via an eNOS- and KATP channel-dependent mechanism. Testing in pigs also demonstrated cardioprotective activity of EP94 [8,9].According to different sources, all three opioid receptor subtypes, μ-, δ- and κ- have been proposed as potential mediators of the cardioprotective effect of exogenous opioids [10]. However, most data confirm the predominant role of δ-receptors in mediating the phenomenon of ischemic preconditioning (IPC) by which brief episodes of myocardial ischemia increase the ability of the heart to tolerate a subsequent prolonged period of ischemic injury [10,11].Myocardial protective properties of the novel enkephalin analogue EP94 as a mimic of IPC and the efficiency of EP94 given during prolonged ischemia and reperfusion has been described in the current study.Materials and Methods
Animal studies were carried out according to protocols approved by the Institutional Animal Care and Use Committee of the Institute of Bioorganic Chemistry (Branch), Pushchino, Moscow Region. The Association for Assessment and Accreditation of Laboratory Animal Care (AAALAC) International accredited Biological Testing Laboratory that conducted the study.Enkephalin analogs EP94 was manufactured by Polypeptide Laboratories France SAS (Strasburg) according to the principles and guidelines of current good manufacturing practice as laid down in the EU guidelines Eudralex GMP Volume 4, Part II, and the US 21 CFR Part 210, 211. Identity and purity of peptide were conformed by Mass spectral analysis and RP-HPLC analysis (Purity=97.7%).
Surgical preparation
Male CD (Sprague-Dawley) rats (280-350 g, Pushchino Breeding Center, Moscow Region) were anesthetized with urethane (1.5 g/kg, intraperitonealy) and placed on the heat pad at 37°C. Following intubation, ventilation was provided using a Rodent Respirator (UGO BASILE, Italy) with atmospheric air at a tidal volume of 10 mL and a rate of 65 cycles/min. The right femoral vein was cannulated to allow administration of drugs and vehicle. A thoracotomy was performed at the fifth intercostal space and the heart was exposed. The pericardium was removed, and the left coronary artery (LCA) was ligated with 5-0 silk sutures. The ends of suture were passed through a small piece of PE-10 tubing to form a snare to occlude the LCA. After 25 minutes or 40 minutes the occlusion was released and the coronary artery was reperfused for 120 minutes.
Measurement of the area at risk and infarct size
At the end of reperfusion, methylene blue dye (0.4 ml of 10% w/v in saline) was injected into the venous catheter to stain the normally perfused region of the heart. The area defined as normal was dyed blue and the total area at risk remained pink. The heart was excised, flushed in distilled water and cut into 2-mm-thick cross-sectional slices. The slices were incubated at 37°C for 15 minutes in a 1% solution of 2,3,5-triphenyltetrazolium chloride (TTC) in 100 mM phosphate buffer (pH 7.4) and immersed in 10% formalin for 5 min. The areas of infarct (TTC negative) and risk zone (TTC stained) were determined by a computerized planimetry technique (Image Tool software). The infarct size (IS), expressed as a percentage of the area at risk (IS/AAR), was taken as a measure of cardioprotection.
Experimental protocols
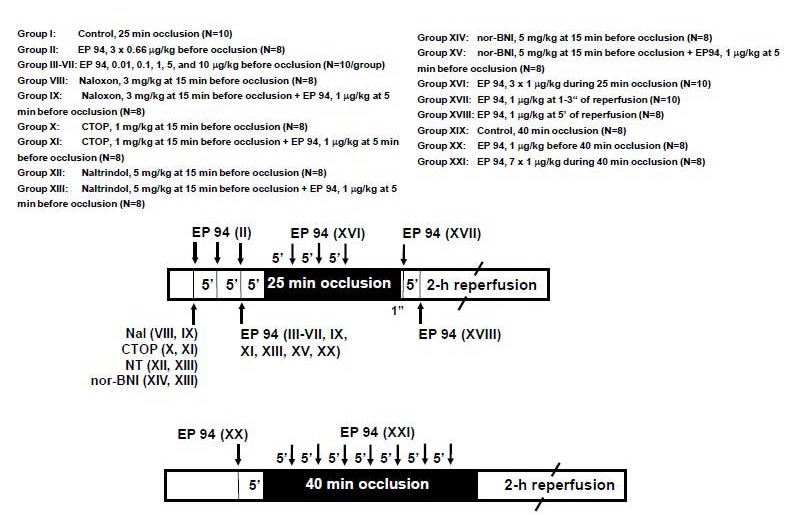
The experimental protocols are outlined in Figure 1. The control groups were subjected to 25 minutes or 40 minutes of coronary LCA occlusion and 2 hours of reperfusion. In the first set of experiments, EP94 was injected (0.66 μg/kg) three times at 15, 10 and 5 minutes before LCA occlusion to mimic ischemic preconditioning or was injected by bolus injection 5 minutes before ischemia in doses of 0.01, 0.1, 1, 5, or 10 μg/kg for dose-response evaluation.In the opioid antagonist studies, rats were administrated the nonselective opioid receptor antagonist Nal (naloxone) (3 mg/kg, iv) or the selective opioid receptor antagonists: CTOP (D-Phe-Cys-Tyr-DTrp-Orn-Thr-Pen-Thr-NH2,) (μ, 1 mg/kg, iv), naltrindole (δ, 5.0 mg/kg, iv) or nor-BNI Norbinaltorphimine) (κ, 5 mg/kg, iv) alone 15 min before LCA occlusion or 10 min before dosing with EP94 (1 μg/kg).To investigate whether EP94 retained cardioprotection with prolonged ischemia and reperfusion, it was injected (1 μg/kg) at 5 minutes before the 25-minute or 40-minute LCA occlusion every 5 minutes during the 25-minute or 40-minute occlusion period or during the first 5 minutes of reperfusion.All agents were administered in a volume of 1 mL/kg as a bolus via the femoral vein. EP94 was dissolved in physiological saline. Figure 1: A schematic diagram of the experimental protocols.
Figure 1: A schematic diagram of the experimental protocols.
Statistical analysis of data
Data analysis was performed with a personal computer-based statistical software package (Prism v.5.0; GraphPad Software, San Diego, CA). Data were expressed as mean ± S.E.M. IS/AAR were analyzed between groups using a one way ANOVA followed by the Tukey post hoc test for multiple comparisons. Statistical significancewas determined at P ≤ 0.05.Results
Cardioprotective effect of EP94 prior to the onset of occlusion
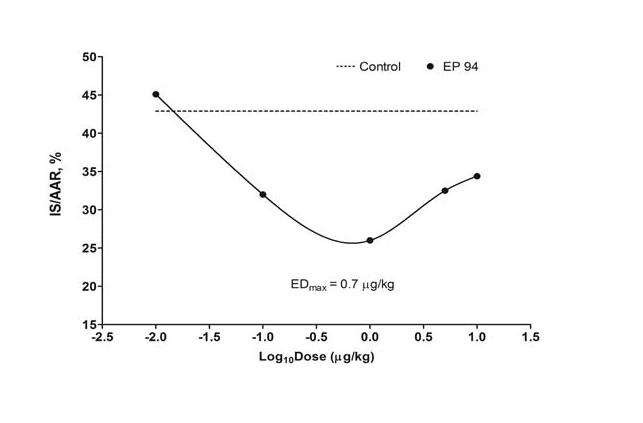
EP94 showed significant cardioprotective activity after a single bolus injection of 1 μg/kg before 25-minute of ischemia and 2-h of reperfusion (26.0 ± 3.5%, P < 0.01 versus control), (Figure 2). The average IS/AAR for the control group was 42.9 ± 2.7%. We discovered that the heart responded in a non-monotonic fashion to exposure to EP94. The U-shaped non-monotonic dose-response curve is presented in Figure 3. High and low doses of EP94 revealed no cardioprotective activity of EP94 relative to control, whereas doses between 0.14 μg/kg and 3.5 μg/kg demonstrated IS/AAR lower than 30%. It is necessary to mention that the experiments with rats revealed that the maximal effective dose was very low (EDmax = 0.7 μg/kg) which could be useful for practical use in a clinical setting. Three consecutive bolus injections (0.66 μg/kg x 3) before ischemia turned out to be even more effective and reduced infarct size to 22.8 ± 1.9% (P < 0.001 versus control, Figure 2). Figure 2: Cardioprotective effect of EP94 during 25 min and 40 min (prolonged) occlusion and reperfusion (iv, 1 μg/kg, bolus injections; except for 0.66 μg/kg x 3 before occlusion). *P < 0.001 vs. Control.Opioid receptor subtypes studies
Figure 2: Cardioprotective effect of EP94 during 25 min and 40 min (prolonged) occlusion and reperfusion (iv, 1 μg/kg, bolus injections; except for 0.66 μg/kg x 3 before occlusion). *P < 0.001 vs. Control.Opioid receptor subtypes studies Figure 3: Dose-response curve for cardioprotective effect (IS/AAR%) of EP94 (i.v. bolus administration 5 min before 25 min occlusion following 2 hours reperfusion).
Figure 3: Dose-response curve for cardioprotective effect (IS/AAR%) of EP94 (i.v. bolus administration 5 min before 25 min occlusion following 2 hours reperfusion).
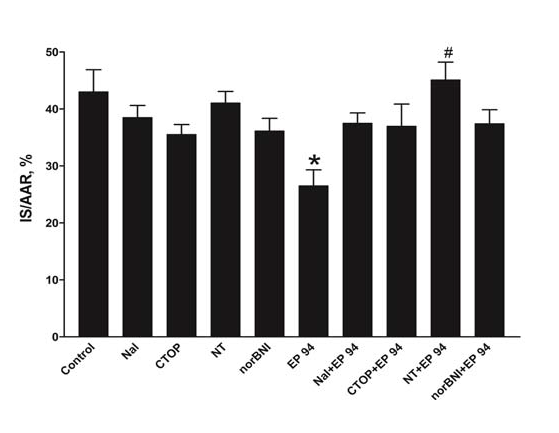
The effect of the nonselective opioid receptor antagonist, naloxone (Figure 1; Group VIII,IX) on the cardioprotective activity of EP94 is presented in Figure 4. These results suggest that the cardioprotective effect of EP94 was a consequence of opioid receptor stimulation, since its beneficial effect was completely inhibited by pre-treatment with the non-selective opioid receptor antagonist, naloxone. The average IS/AAR in group Nal+EP94 was 37,5 ± 1.8%. We used selective opioid antagonists CTOP (μ-), naltrindole (δ-) and nor-BNI (κ-) to determine which subtype of opioid receptor was responsible for EP94-induced preconditioning. All antagonists were effective at blocking the cardioprotective effect of EP94. There were no significant reduction in IS/AAR versus control when CTOP, naltrindole or nor-BNI were administrated followed by injection of EP94 (45,1 ± 3.1%.: 37,0 ± 3.9%.: 37,4 ± 2.4% respectively). However, it should be noted that the δ-antagonist, naltrindole, was slightly more effective, and its pre-treatment significantly blocked the effect of EP94 completely. Administration of antagonist without peptide did not alter the size ratio IS/AAR in groups.Cardioprotective effect of EP94 during 25-minutes and 40-minutes (prolonged) occlusion and reperfusion Figure 4: Cardioprotective effect of EP94 during 25 min and 40 min (prolonged) occlusion and reperfusion (iv, 1 μg/kg, bolus injections; except for 0.66 μg/kg x 3 before occlusion). *P < 0.001 vs. Control.
Figure 4: Cardioprotective effect of EP94 during 25 min and 40 min (prolonged) occlusion and reperfusion (iv, 1 μg/kg, bolus injections; except for 0.66 μg/kg x 3 before occlusion). *P < 0.001 vs. Control.
Repeated (every 5 min) bolus injections of EP94 during the 25-minutes of ischemia effectively reduced the IS/AAR to 27.3 ± 1.0% versus 42.9 ± 2.7% in control group, P < 0.001 (Figure 2). The multiple injection protocol of EP94 administration maintains its high cardioprotective activity despite the prolongation of ischemia to 40 minutes. EP94 injected before 40-minute LCA occlusion did not alter infarct size (55.2 ± 2.6% versus 52.2 ± 1.8% in control group). However, repeated (every 5 min) EP94 administration after start of occlusion caused significant cardioprotection (34.8 ± 1.8%, P < 0.001, Figure 2).Whether EP94 could protect rat hearts during reperfusion, we administrated EP94 (1 μg/kg) during the first 5 minutes of LCA reperfusion. Although EP94 was protective when given before or during ischemia, it failed to decrease infarct size when given at reperfusion in the present study. There were no noticeable effects of EP94 on reduction of infarct size when peptide was administrated in the first seconds or minutes of reperfusion (36.8 ± 1.9% and 42.6 ± 1.7% respectively versus 42.9 ± 2.7% in control group, Figure 2).Discussion
The cardioprotective activity of the novel enkephalin, analogue EP94, has been demonstrated by studies performed in several laboratories when administered prior to occlusion or during occlusion. Previously, Karlsson et al. have demonstrated a reduction of infarct size produced by EP94 administration in different porcine models of myocardial ischemia and reperfusion [8,9]. The protective effect of EP94 is at least partially the result of activation of nitric oxide synthase and adenosine triphosphate potassium channel-dependent mechanism [7]. Further studies with selective opioid antagonists demonstrated that the cardioprotective effect of EP94 injected during ischemia in rats is mediated primarily via activation of centrally located μ opioid receptors [12].The current study was performed to determine whether EP94 can mimic the phenomenon of ischemic preconditioning (IPC) [13], similar to previously studied opioid agonists [14-16] and if so, which opioid receptor mediates this effect. Three repetitive administrations of EP94 prior to the onset of a 25-minute occlusion considerably reduced the infarct size when followed by 2 hr of reperfusion. The effect appeared to be dose-related at 0.1-10 μg/kg. It is important to stress that the experiments in rats revealed that the effective dose of EP94 turned out to be very low when compared with the known clinically available opioid agonist, morphine [17,18], the opiate that has been most extensively studied in cardioprotection.There is a growing body of evidence that one of the three known opioid receptors, e.g., the δ-opioid receptor, mediates early IPC [15,17]. Naturally, the hypothesis to be tested to determine whether the δ-receptors are the more likely candidate of opioid receptors involved in the preconditioning phenomenon by EP94 should be tested. EP94 is an enkephalin analogue with high affinity for the μ-opioid receptor subtype, lower affinity for the δ-opioid receptor and to a less extent for the κ-opioid receptor (unpublished data). The protective effect of EP94 was abolished by coadministration of EP94 not only with naltrindole (δ-opioid receptor antagonist), but also with selective μ-, and κ-opioid receptor antagonists.The results of the present study further suggest that pharmacological preconditioning with EP94 can confer acute cardioprotection via activation of all opioid receptors. Nevertheless, we should like to mention, that the blocking action of naltrindole in our experiments has a more significant effect and it is in agreement with the results of other authors concerning the role of the δ-opioid receptor in IPC.In a previous study of Gross et al. [12] suggested that EP94 injected during ischemia reduced infarct size in rat hearts via activation of centrally located μ-opioid receptors. The μ-opioid receptor has traditionally been believed to be absent from adult rat myocytes, based on binding studies [19,20]. The lack of μ-opioid receptor activity in the cardioprotective effect of IPC has also been supported by a number of functional studies, indicating an absence of this particular opioid receptor in rat myocytes [19,21].Quite possibly, the cardioprotective effect of systemically administrated opioids can be through the simultaneous activation of peripheral and central opioid receptors. According to different sources, the cardioprotective effect of exogenous opioids can be attributed through activation of cardiac δ- and κ- receptors, as well as through extracardiac localized μ, δ- and κ- receptors [18,22-26].In the present study the selective δ-opioid receptor antagonist, naltrindole, attenuated the infarct sparring effect of EP94. These results are in accordance with the known data which suggests that stimulation of the δ-opioid receptor by IPC or pharmacological imitation of IPC by opioids appears to protect heart muscle from ischemia [15,17]. It is necessary to take into account the basic condition of the endogenous opioid system for better understanding the mechanism of action of the novel enkephalin analogue in case of administration of EP94 prior occlusion (current work) or during occlusion [12]. It is well documented that the level of specific cardiac opioids are elevated in response to myocardial ischemia [27]. Presumably, released endogenous enkephalins bind mainly to the δ-cardiac opioid receptors and can influence the receptor preference to exogenous opioids administrated in such conditions. We have been using EP94 in our experiments and assume, that EP94 administrated before ischemia can protect the rat heart via activation of all three opioid receptors: the δ - and κ- cardiac opioid receptors and μ-opioid receptors with extracardiac localization.In the next part of our work we focused on the effects of EP94 in a rat model with a more prolonged occlusion period. One time administration of EP94 in the dose of 1 μg/kg to rats in experiments with 40 min occlusion instead of 25 min occlusion failed to show the protective effect of EP94, whereas multiple (every 5 min) injections of EP94 during the total period of occlusion not only preserved the cardioprotective effect of EP94, but demonstrated considerable reduction of infarct size by 30% in such severe conditions. This prolonged effect obtained with EP94 may be useful in heart surgery in cases of complicated, long-term heart operations. It will give more time to a physician to proceed with reperfusion therapy to patients in an acute myocardial infarction treatment when the time frame is very important. Multiple injections of EP94 could extend this timeEP94 activity at reperfusion has been tested, as well. We have not found a reduction of infarct size when EP94 was administrated in the first seconds or minutes of reperfusion. In a previous study, EP94 administrated by an intracoronary infusion (0.2 μg/kg/min) maintained for the last 10 minutes of ischemia and start of reperfusion reduced infarct size in open-chest pigs [8]. However, the cardioprotection was not present when EP94 was administered by single injection late during ischemia at doses up to 25 μg/kg in closed-chest pigs [9].The concordance of animal models is one of the important problems concerning the pre-clinical setting. The μ-opioid receptor are thought to be absent in adult rat cardiomyocytes, whereas δ-and κ-opioid receptors are expressed [19,20]. Similar results were obtained in pig hearts [9]. This is quite different from the human heart, where both μ- and δ- opioid receptors are present [28].Finally we should like to emphasize the safety of EP94. There were no deaths of animals observed under control conditions when doses up to 100 mg/kg in safety tests of toxicity. No difference in any of the hemodynamic parameters between control and treatment groups undergoing ischemia and reperfusion in doses of EP94 up to 10 mg/kg were observed in experiments carried out in this work (unpublished data).Taken together, the data suggest that the cardioprotective activity of EP94 tested on the infarction rat model may be beneficial for the treatment of myocardium resistance during ischemia.Conclusion
In summary, we demonstrated the dose-related reduction of cardioprotective effects of EP94 administrated intravenously prior ischemia in rats. μ-,δ-,κ-opioid receptors were involved in cardioprotection of EP94 administrated prior ischemia. It was found that the peptide EP94 can mimic the phenomenon of IPC. EP94 turned out to be active at prolongated ischemia. Multiple administrations of EP94 protected the heart during prolongated occlusion that can be useful in infarct treatment. EP94 was ineffective if it was administrated at first seconds or minutes of reperfusion.References
- Kuzume K, Wolff RA, Amakawa K, Kuzume K, Van Winkle DM (2003) Sustained exogenous administration of Met5-enkephalin protects against infarction in vivo. Am J Physiol Heart Circ Physiol 285: H2463-H2470.
- Song W, Shin J, Lee J, Kim H, Oh D, et al. (2005) A potent opiate agonist protects against myocardial stunning during myocardial ischemia and reperfusion in rats. Coron Artery Dis 16: 407-410.
- Bobrova I, Nikiforovich G, Balodis J, Abissova N, Vegners R, et al. (1985) Design of enkephalin analogues. In: Peptides in the nervous system. GDR Reinhardsbrunn, 14-33.
- Bobrova I, Abissova N, Mishlakova N, Rozentals G, Chipens G (1998) Synthesis and biological activity of branched enkephalin analogues. Eur J Med Chem 33: 255-266.
- Bobrova I, Mishlakova N, Selander A, Mekshun E, Rozental G (1998) Synthesis and biological activity of branched enkephalin analogues containing two amino acids in a side chain. Eur J Med Chem 33: 331-334.
- Bobrova I (2008) Cardioprotective compounds. Patent WO/2008/020802 A1.
- Gross GJ, Hsu A, Nithipatikom K, Pfeiffer AW, Bobrova I, et al. (2012) Acute and chronic cardioprotection by the enkephalin analogue, Eribis peptide 94, is mediated via activation of nitric oxide synthase and adenosine triphosphateregulated potassium channels. Pharmacology 90 : 110-116.
- Karlsson LO, Grip L, Bissessar E, Bobrova I, Gustafsson T, et al. (2011) Opioid receptor agonist Eribis peptide 94 reduces infarct size in different porcine models for myocardial ischaemia and reperfusion. Eur J Pharmacol 651: 146-151.
- Karlsson LO, Bergh N, Li L, Bissessar E, Bobrova I, et al. (2012) Dose-dependent cardioprotection of enkephalin analogue Eribis peptide 94 and cardiac expression of opioid receptors in a porcine model of ischaemia and reperfusion. Eur J Pharmacol 674: 378-383.
- Gross GJ, Peart JN (2007) Opioids and myocardial reperfusion injury. Arch Mal Coeur Vaiss 100: 231-237.
- Murry CE, Jennings RB, Reimer KA (1986) Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation 74: 1124-1136.
- Gross G, Hsu A, Nithipatikom K, Bobrova I, Bissessar E (2012) Eribis Peptide 94 Reduces Infarct Size in Rat Hearts Via Activation of Centrally Located μ Opioid Receptors. J Cardiovasc Pharmacol 59: 194-197.
- Gross GJ (2003) Role of opioids in acute and delayed preconditioning. J Mol Cell Cardiol 35: 709-718.
- Schultz JE, Hsu AK, Gross GJ (1996) Morphine mimics the cardioprotective effect of ischemic preconditioning via a glibenclamide-sensitive mechanism in the rat heart. Circ Res 78: 1100-1104.
- Fryer RM, Hsu AK, Eells JT, Nagase H, Gross GJ (1999) Opioid-induced second window of cardioprotection: potential role of mitochondrial KATP channels. Circ Res 84: 846-851.
- Peart JN, Gross ER, Gross GJ (2005) Opioid-induced preconditioning: recent advances and future perspectives. Vascul Pharmacol 42: 211-218.
- Schultz JJ, Hsu AK, Gross GJ (1997) Ischemic preconditioning and morphineinduced cardioprotection involve the delta (delta)-opioid receptor in the intact rat heart. J Mol Cell Cardiol 29: 2187-2195.
- Li R, Wong GT, Wong TM, Zhang Y, Xia Z, et al. (2009) Intrathecal morphine preconditioning induces cardioprotection via activation of delta, kappa, and mu opioid receptors in rats. Anesth Analg 108: 23-29.
- Zimlichman R, Gefel D, Eliahou H, Matas Z, Rosen B, et al. (1996) Expression of opioid receptors during heart ontogeny in normotensive and hypertensive rats. Circulation 93: 1020-1025.
- Ventura С, Spurgeon H, Lakatta EG, Guarnieri C, Capogrossi MC (1992) Kappa and delta opioid receptor stimulation affects cardiac myocyte function and Ca2+ release from an intracellular pool in myocytes and neurons. Circ Res 70: 66-81.
- Ela C, Barg J, Vogel Z, Hasin Y, Eilam Y (1997) Distinct components of morphine effects on cardiac myocytes are mediated by the kappa and delta opioid receptors. J Mol Cell Cardiol 29: 711-720.
- Schultz JE, Hsu AK, Gross GJ (1998) Ischemic preconditioning in the intact rat heart is mediated by delta1- but not mu- or kappa-opioid receptors. Circulation 97: 1282-1289.
- Fryer RM, Wang Y, Hsu AK, Nagase H, Gross GJ (2001) Dependence of delta1-opioid receptor-induced cardioprotection on a tyrosine kinasedependent but not a Src-dependent pathway. J Pharmacol Exp Ther 299: 477-482.
- Peart JN, Gross GJ (2004) Exogenous activation of delta- and kappa-opioid receptors affords cardioprotection in isolated murine heart. Basic Res Cardiol 99: 29-37.
- Maslov LN, Lishmanov YB, Oeltgen PR, Barzakh EI, Krylatov AV, et al. (2009) Activation of peripheral delta2 opioid receptors increases cardiac tolerance to ischemia/reperfusion injury. Involvement of protein kinase C, NO-synthase, KATP channels and the autonomic nervous system. Life Sci 84: 657-663.
- Zhang Y, Irwin MG, Wong TM, Chen M, Cao CM (2005) Remifentanil preconditioning confers cardioprotection via cardiac kappa- and delta-opioid receptors. Anesthesiology 102: 371-378.
- Schulz R, Gres P, Heusch G (2001) Role of endogenous opioids in ischemic preconditioning but not in short-term hibernation in pigs. Am J Physiol Heart Circ Physiol 280: H2175-H2181.
- Villemagne PS, Dannals RF, Ravert HT, Frost JJ (2002) PET imaging of human cardiac opioid receptors. Eur J Nucl Med Mol Imaging 29: 1385-1388.