
Case Report
*Address for Correspondence: Ashraf M Aly, MD, PhD, MSc, FACC, FAAP, Professor of Pediatrics and Maternal Fetal Medicine, Director, Pediatric and Fetal Cardiology, University of Texas, 2.210 Research Building 6, 301 University Boulevard, Galveston, Texas, 77555-0361, USA, Tel: (409) 772-2507; Fax: (409) 772-5045; E-mail: amaly@utmb.edu
Citation: Hill C, Lindsay D, Aly A. Dextrocardia with Situs Inversus, Atrio-ventricular and Ventricular-arterial Concordance and a Left Posterior Aorta in a Preterm Twin Neonate. J Pediatr Child Care. 2015;1(2): 3.
Copyright © 2015 Aly et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 2
Submission: 11 August, 2015 | Accepted: 12 October, 2015 | Published: 17 October, 2015
 An echocardiogram showed a mirror image dextrocardia with inversion of both atria and ventricles (Figure 2). The great arteries were also inverted with the pulmonary artery connected to a morphologic right ventricle on the left (Figure 3), and the aorta connected to a morphologic left ventricle on the right (Figure 4). There was a rightsided aortic arch as shown by the direction of the arch and its first bifurcating branch (Figure 4). The aortic valve was noted to be on the left and slightly posterior to the pulmonary valve (Figure 5). A small secundum type atrial septal defect (ASD) was also noted. The left ventricular function was normal. No other cardiac malformations were detected. Both twins A and B stayed in the NICU for 3 weeks primarily for feeding problems related to their prematurity and were then discharged home in a good health.
An echocardiogram showed a mirror image dextrocardia with inversion of both atria and ventricles (Figure 2). The great arteries were also inverted with the pulmonary artery connected to a morphologic right ventricle on the left (Figure 3), and the aorta connected to a morphologic left ventricle on the right (Figure 4). There was a rightsided aortic arch as shown by the direction of the arch and its first bifurcating branch (Figure 4). The aortic valve was noted to be on the left and slightly posterior to the pulmonary valve (Figure 5). A small secundum type atrial septal defect (ASD) was also noted. The left ventricular function was normal. No other cardiac malformations were detected. Both twins A and B stayed in the NICU for 3 weeks primarily for feeding problems related to their prematurity and were then discharged home in a good health.




Dextrocardia with Situs Inversus, Atrio-ventricular and Ventriculararterial Concordance and a Left Posterior Aorta in a Preterm Twin Neonate
Chelsea Hill, David Lindsay and Ashraf Aly*
- Department of Pediatrics, Division of Pediatric Cardiology, University of Texas Medical Branch, 301 University Blvd, Galveston, TX, 77555, USA
*Address for Correspondence: Ashraf M Aly, MD, PhD, MSc, FACC, FAAP, Professor of Pediatrics and Maternal Fetal Medicine, Director, Pediatric and Fetal Cardiology, University of Texas, 2.210 Research Building 6, 301 University Boulevard, Galveston, Texas, 77555-0361, USA, Tel: (409) 772-2507; Fax: (409) 772-5045; E-mail: amaly@utmb.edu
Citation: Hill C, Lindsay D, Aly A. Dextrocardia with Situs Inversus, Atrio-ventricular and Ventricular-arterial Concordance and a Left Posterior Aorta in a Preterm Twin Neonate. J Pediatr Child Care. 2015;1(2): 3.
Copyright © 2015 Aly et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Pediatrics & Child Care | ISSN: 2380-0534 | Volume: 1, Issue: 2
Submission: 11 August, 2015 | Accepted: 12 October, 2015 | Published: 17 October, 2015
Abstract
In dextrocardia, the main base-apex cardiac axis is directed to the right side of the chest. The majority of dextrocardia is associated with situs solitus and either normally related or L-transposed great vessels. Dextrocardia with situs inversus is rare and presents in different forms depending on the atrio-ventricular (AV) and ventricular-aterial (VA) relationship. We report a rare case of dextrocardia with situs inversus, AV and VA concordance, a left posterior aorta and a right aortic arch in a preterm twin male infant.Keywords
Dextrocardia; Situs inversus; Ventricular inversionIntroduction
The main cardiac axis (base to apex) determines the orientation of the heart in the chest. In dextrocardia, the axis points to the right instead of the left [1-4]. This differs from dextro position where the heart is positioned in the right side of the chest secondary to a pathologic process, but retains the normal axis [4]. Dextrocardia may occur as an isolated defect or may be associated with cardiac, vascular and/or visceral abnormalities. The relationship between the atria and viscera may present in one of three possible forms: situs solitus, situs inversus, or situs ambiguous. Situs solitus is the usual anatomy with the right atrium and the liver on right, and the stomach on the left. Situs inversus describes reversal of the viscera with the right atrium and the liver on the left and the stomach and the spleen on the right. Situs ambiguous, also called heterotaxy, describes an indeterminate situs and is usually associated with either asplenia or polysplenia. The ventricles may be concordant or discordant with their corresponding atria. The great arteries may be normally related, inversely related (mirror image), or transposed [5].Case Report
A 32-week twin a male infant, weighing 1810 grams, was born to a 32 year-old G5P1 mother. This was a di-di twin pregnancy with IUGR in twin B. The pregnancy was complicated by in-vitro fertilization, gestational diabetes, hypothyroidism “on levothyroxine”, preeclampsia “on magnesium sulfate”, and preterm labor. The mother underwent C-section due to worsening pre-eclampsia. Both twins were given basic neonatal care. APGARs cores were 8 and 9 at 1 and 5 minutes, respectively. They had stable vital signs with oxygen saturation of 97% on room air. While twin B had a normal examination, twin A was incidentally noted to have heart sounds on the right side of the chest. No murmurs were appreciated. A chest X-ray (Figure 1) revealed dextrocardia with situs inversus, which was further confirmed by an abdominal ultrasound.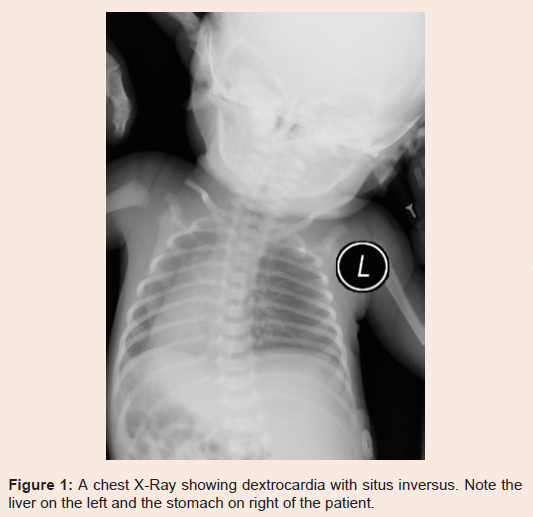
Figure 1: A chest X-Ray showing dextrocardia with situs inversus. Note the liver on the left and the stomach on right of the patient.
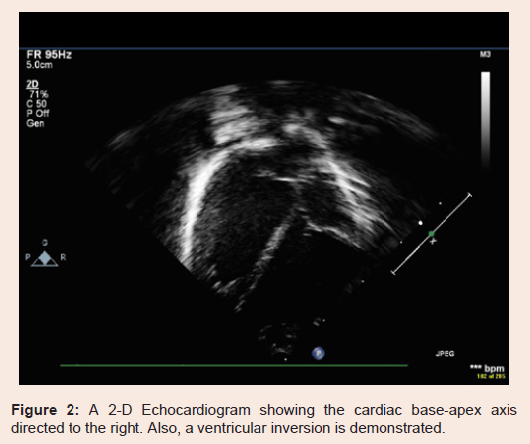
Figure 2: A 2-D Echocardiogram showing the cardiac base-apex axis directed to the right. Also, a ventricular inversion is demonstrated.
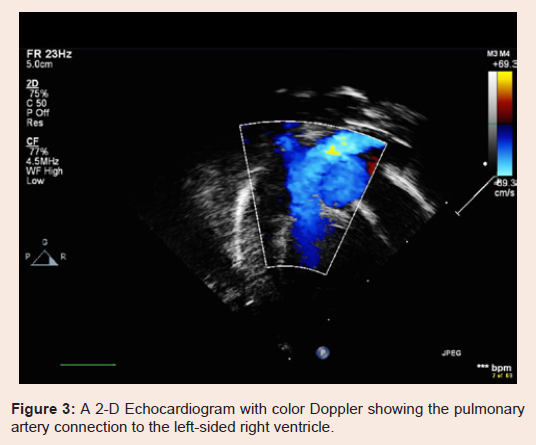
Figure 3: A 2-D Echocardiogram with color Doppler showing the pulmonary artery connection to the left-sided right ventricle.
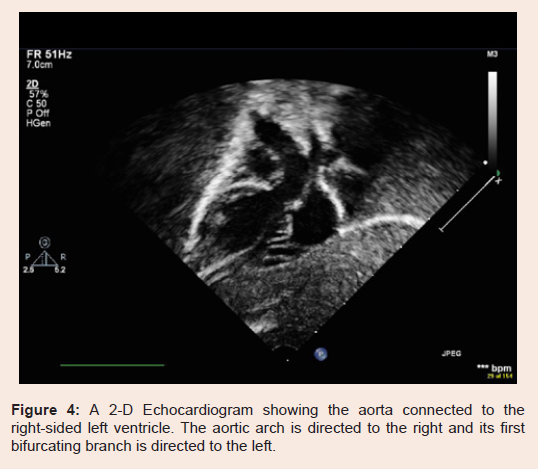
Figure 4: A 2-D Echocardiogram showing the aorta connected to the right-sided left ventricle. The aortic arch is directed to the right and its first bifurcating branch is directed to the left.
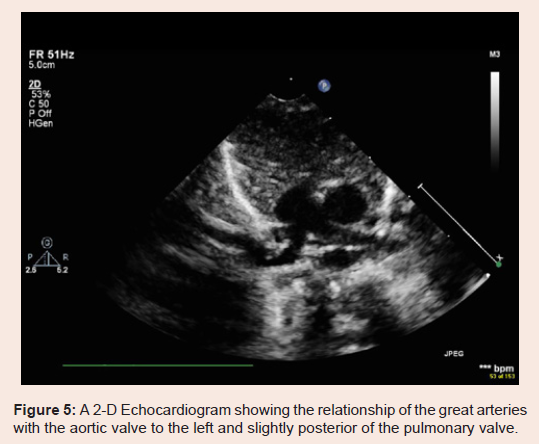
Figure 5: A 2-D Echocardiogram showing the relationship of the great arteries with the aortic valve to the left and slightly posterior of the pulmonary valve.
Discussion
The exact incidence of dextrocardia is not known, however one study reported it to be 1 in 12,019 pregnancies in the general population [6]. In another study, the incidence of dextrocardia was found to be 1 of 455 high-risk pregnancies in women undergoing fetal echocardiography for possible congenital heart defects (CHD). In the same study, situs solitus was found in 47%, situs ambiguous in 30%, and situs inversus in 23% of the cases [4]. Another study reported dextrocardia to be associated with situs solitus in 64%, situs inversus in 27%, and situs ambiguous in 9% [2]. In our case report, the patient was incidentally found to have dextrocardia, situs inversus, concordant atrio-ventricular and ventricular-arterial connections, and a left posterior aortic valve.Except for a small secundum ASD, our patient had no other CHD. Situs solitus dextrocardia is known to be more associated with CHD than situs inversus. In one study, situs solitus was associated with CHD in 93% of the cases, with left to right shunts being the most common (40.9%) followed by conotruncal defects (36.4%) [3]. The reported incidence of CHD associated with situs inversus dextrocardia ranges from 23-71.4% [3,6]. L-transposition was reported in 66.7% of the cases. Those patients are usually asymptomatic as long as there are no other associated heart defects [3]. This may explain why these cases may be under-reported in the general population [3,7].
Conclusion
We describe a rare case of dextrocardia with situs inversus, atrioventricular and ventricular-arterial concordance and a left posterior aorta in an infant. This was an incidental finding since the patient had no cardiac symptoms as the cardiac hemodynamics was normal.References
- Squarcia U, Ritter DG, Kincaid OW (1973) Dextrocardia: angiocardiographic study and classification. Am J Cardiol 32: 965-977.
- Huhta JC, Hagler DJ, Seward JB, Tajik AJ, Julsrud PR, et al. (1982) Two-dimensional echocardiographic assessment of dextrocardia: a segmental approach. Am J Cardiol 50: 1351-1360.
- Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N (2003) Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol 88: 143-155.
- Bernasconi A, Azancot A, Simpson JM, Jones A, Sharland GK (2005) Fetal dextrocardia: diagnosis and outcome in two tertiary centers. Heart 91: 1590-1594.
- Van Praagh R, Van Praagh S, Vlad P, Keith JD (1964) Anatomic types of congenital dextrocardia diagnostic and embryologic implications. Am J Cardiol 13: 510-531.
- Bohun CM, Potts JE, Casey BM, Sandor GG (2007) A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol 100: 305-309.
- O'Leary PW, Hagler DJ (2013) Cardiac malpositions and abnormalities of atrial and visceral situs. In: Allen HD, Driscoll DJ, Shaddy RE, Feltes TF (eds). Moss and adams heart disease in infants, children, and adolescents: including the fetus and young adult, (8th edn), Vol. II. Lippincott Williams & Wilkins, Wolters Kluwer Business, Philadelphia, USA, pp. 1195-1207.
- Van Praagh R, Van Praagh S, Vlad P, Keith JD (1965) Diagnosis of the anatomic types of congenital dextrocardia. Am J Cardiol 15: 234-247.