
Journal of Surgery
Download PDF
Special Issue: Surgical Oncology
Case Report
*Address for Correspondence: Jan Jacobs, M.D., Department of General, Visceral, Trauma and Thoracic Surgery, Hospital of Ludwigshafen, Bremserstr. 79, 67063 Ludwigshafen am Rhein, Germany, Tel: +49 (0)621 503-3150; Fax: +49 (0) 621 503-3184; E-mail: cha@klilu.de
Citation: Hirche Z, Hirche C, Kremer T, Kneser U, Willis S, et al. Phylloides Tumors of the Breast: A Case Series with Review of the Literature. J Surgery. 2015; S(2): 6.
Copyright © 2015 Hirche Z, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 2
Submission: 18 April 2015 | Accepted: 02 June 2015 | Published: 06 June 2015
Editors:Dr. Marlon A Guerrero, Assistant Professor of Surgery, University of Arizona, USADr. James A Warneke, Associate Professor of Surgery, University of Arizona, USA
Patient and method: A Medline analysis was performed to extract recent literature on PT. The review of the literature was matched with a retrospective analysis of all PT cases treated between 2003 and 2012 in our hospital. The analysis included PT characteristics and histology, surgical procedures and an outcome evaluation. A case demonstration was included to visualize an extreme rare and challenging, infiltrating PT.
Results: In our study, 2 out of 9 patients suffered from benign PT (BPT) (22.2%), one from borderline PT (BLPT) (11.1%) and six from malignant PT (MPT) (66.7%). The tumor size ranged from 2.5 to 4 cm for BPT, 1.5 cm for BPLT and 4.5 to 23 cm for MPT. Six patients underwent local excision, while 2 patients were treated with mastectomy and one patient required individualized surgery by a multi surgical approach with radical tumor resection and plastic surgical reconstruction. This complex case is demonstrated separately. All nine patients underwent surgery with disease-free margins (100%). The review of the literature revealed no existing guidelines for the treatment of PT, thus the therapeutical management remains without standardization. There is consensus, that surgery is the 1st line therapy of PT and ranges from local excision, mastectomy to radical, wide resections. The inalienable factor for prognosis appears to be a margin-free-resection > 1 cm.
Conclusion: Only in rare cases, complex and individualized, multi surgical approaches with plastic surgical reconstruction are necessary for PT. While most cases are seen as MPT, even BPT and BLPT tend to malignant transformation, local recurrence and systemic spread. Treatment requires an individual approach due to the varying biological features and tumor size. From literature perspective, diseasefree specimen margins are the prime principle for all PT subtypes to achieve optimal oncological treatment.
We performed a retrospective analysis of patients between 2003 and 2012 (10 years), who were diagnosed with PT and underwent treatment at our institution. Medical records of these patients were reviewed and clinical characteristics retrieved, included gender, age, oncological features of PT including tumor size and tumor location, type of surgery, histological data regarding subtype of PT and diseasefree margins, survival rate, morbidity and mortality (Table 1). DefinitionsHistopathology: The final diagnosis of PT was based on the histological criteria analogue to Elston and Elli: PT were divided into benign (BPT), borderline (BLPT), or malignant (MPT) PT [9].1) Local excision, characterized by a margin-free removal of the tumor, whereas the disease-free margin is <1.0 cm.2) Wide excision, characterized by a margin-free removal of the tumor, whereas the disease-free margin is >1.0.3) Mastectomy, subdivided into simple, total or radical mastectomy.4) Individualized radical wide tumour resection, p.r.n with reconstructionThe indication for the type of surgical procedure was based on preoperative imaging with regard to tumor extend and/or invasive growth. If a pretherapeutic core needle biopsy was performed and BLPT or MPT were histologically approved, staging investigations including abdominal ultrasound and chest X-ray were perfomed routinely, while CT-scan and skeletal scintigraphy were indicated on an individual basis.
DefinitionsHistopathology: The final diagnosis of PT was based on the histological criteria analogue to Elston and Elli: PT were divided into benign (BPT), borderline (BLPT), or malignant (MPT) PT [9].1) Local excision, characterized by a margin-free removal of the tumor, whereas the disease-free margin is <1.0 cm.2) Wide excision, characterized by a margin-free removal of the tumor, whereas the disease-free margin is >1.0.3) Mastectomy, subdivided into simple, total or radical mastectomy.4) Individualized radical wide tumour resection, p.r.n with reconstructionThe indication for the type of surgical procedure was based on preoperative imaging with regard to tumor extend and/or invasive growth. If a pretherapeutic core needle biopsy was performed and BLPT or MPT were histologically approved, staging investigations including abdominal ultrasound and chest X-ray were perfomed routinely, while CT-scan and skeletal scintigraphy were indicated on an individual basis.
Literature review
We conducted a systematic literature research in Medline, using the terms “phylloides tumors”, “cystosarcoma phylloides” and “breast mass”.Analysis of each reference included objectification of the total number of included patients, local recurrence rate, rate of metastatic spread, surgical approach and application of adjuvant radiation or chemotherapy (Table 2). Some studies enabled separated evaluation of tumor subtype (BPT, BLPT and MPT) was possible. All further results from literature review are displayed in Table 2. Ethics statementAccording to the local ethics committee based on the declaration of Helsinki, further ethical consultation and approval was not necessary, because only routine data based were anonymously analysed without further intervention.
Ethics statementAccording to the local ethics committee based on the declaration of Helsinki, further ethical consultation and approval was not necessary, because only routine data based were anonymously analysed without further intervention.
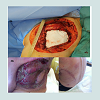
Retrospective chart review revealed 9 eligible cases of female patients with PT treated between 2003 and 2013. The mean age was 62 years, ranging from 45-83 years. Histological evaluation revealed 2 out of 9 patients suffering from BPT (22.2%), one from BLPT (11.1%) and 6 from MPT (66.7%) (Table 1). The size of the tumors ranged from 2.5 to 4 cm for BPT, 1.5 cm for BPLT and 4.5 to 23 cm for MPT. All patients primarily received a surgical treatment under curative intention (Table 1). Six patients underwent a local excision, hereunder two cases with a BPT, one with a BLPT and 3 with a MPT histologically. Two patients, who suffered from MPT, underwent a mastectomy. The MPT patient with a diameter of 23 cm was a rare and complex case which required multi surgical management with individualized radical wide tumour resection by radical mastectomy and partial chest wall resection followed by reconstruction with alloplastic mesh, a regional transposition flap and mesh graft transplantation. This case is further summarized and displayed in Figures 1-4.

 All patients underwent surgery with disease-free margins (100%). With a postoperative mortality rate of 0%, no minor or major surgical complications occurred (0%).In three cases with MPT, adjuvant radiotherapy was performed (Table 1): Two patients received postoperative radiotherapy because of safety margin <1 cm. One patient received postoperative radioand chemotherapy simultaneously, because of coincidentally diagnosed breast cancer. Seven patients were lost to follow-up. Only two patients, who suffered from MPT, could be re-evaluated. In both cases no local recurrence or metastatic spread was found (Table 1). Follow-up time was 6 and 16 months.Literature reviewMost available studies on PT between 1951 and 2014 have a retrospective design with analysis of clinicopathological data. Renner and co-workers performed a computer assisted survey from April 2000 to June 2001, which was carried out in 24 surgical and gynaecological departments in Austria [11]. They collected information on PT-treatment, follow-up care and long-term results [11]. They concluded, that also patients with borderline and benign lesions should be scheduled for regular follow-ups [11]. A breast-conserving operation with disease-free margins of the specimen should be the primary objective, since even malignant tumours seldom metastasize [11]. A prospective, multi-institutional study prospectively enrolled patients who were treated with a margin-negative breast-conserving resection for BLPT or MPT and adjuvant radiotherapy [12]. Barth and co-workers concluded, that margin-negative resection combined with adjuvant radiotherapy was an effective therapy to locally control BLPT and MPT [12].Eligible studies revealed a rate of local recurrence of 2-29% in total; 4-27% in BPT, 0-38% in BLPT and 18-50% in MPT [5,7,9,13-20] (Table 2). A higher rate of local recurrence was predominantly seen for MPT compared with BPT in some studies [7,13,16,17]. Rate of metastatic spread ranged from 0-22% in total; 0% in BPT, 0-9% in BLPT and 0-50% in MPT [5,7,9,11,13-20] (Table 2). All studies demonstrated the highest risk for metastatic spread in MPT, compared with BPT or BLPT. In contrast, in their series of 34 patients, Kario and co-workers as well as Moffat and co-workers observed no metastatic spread in MPT after treatment. Regarding surgical therapy, local recurrence rate after excision was higher than after mastectomy [7,14,16,19].
All patients underwent surgery with disease-free margins (100%). With a postoperative mortality rate of 0%, no minor or major surgical complications occurred (0%).In three cases with MPT, adjuvant radiotherapy was performed (Table 1): Two patients received postoperative radiotherapy because of safety margin <1 cm. One patient received postoperative radioand chemotherapy simultaneously, because of coincidentally diagnosed breast cancer. Seven patients were lost to follow-up. Only two patients, who suffered from MPT, could be re-evaluated. In both cases no local recurrence or metastatic spread was found (Table 1). Follow-up time was 6 and 16 months.Literature reviewMost available studies on PT between 1951 and 2014 have a retrospective design with analysis of clinicopathological data. Renner and co-workers performed a computer assisted survey from April 2000 to June 2001, which was carried out in 24 surgical and gynaecological departments in Austria [11]. They collected information on PT-treatment, follow-up care and long-term results [11]. They concluded, that also patients with borderline and benign lesions should be scheduled for regular follow-ups [11]. A breast-conserving operation with disease-free margins of the specimen should be the primary objective, since even malignant tumours seldom metastasize [11]. A prospective, multi-institutional study prospectively enrolled patients who were treated with a margin-negative breast-conserving resection for BLPT or MPT and adjuvant radiotherapy [12]. Barth and co-workers concluded, that margin-negative resection combined with adjuvant radiotherapy was an effective therapy to locally control BLPT and MPT [12].Eligible studies revealed a rate of local recurrence of 2-29% in total; 4-27% in BPT, 0-38% in BLPT and 18-50% in MPT [5,7,9,13-20] (Table 2). A higher rate of local recurrence was predominantly seen for MPT compared with BPT in some studies [7,13,16,17]. Rate of metastatic spread ranged from 0-22% in total; 0% in BPT, 0-9% in BLPT and 0-50% in MPT [5,7,9,11,13-20] (Table 2). All studies demonstrated the highest risk for metastatic spread in MPT, compared with BPT or BLPT. In contrast, in their series of 34 patients, Kario and co-workers as well as Moffat and co-workers observed no metastatic spread in MPT after treatment. Regarding surgical therapy, local recurrence rate after excision was higher than after mastectomy [7,14,16,19].
Phylloides Tumors of the Breast: A Case Series with Review of the Literature
Zarah Hirche1, Christoph Hirche2,3, Thomas Kremer2,3, Ulrich Kneser2,3, Stefan Willis1 and Jan Jacobs1*
- 1Department of General, Visceral, Trauma and Thoracic Surgery, Hospital of Ludwigshafen, Ludwigshafen am Rhein, Germany
- 2Department of Hand, Plastic, and Reconstructive Surgery, Trauma Center Ludwigshafen, Germany
- 3Department of Plastic and Hand Surgery, University of Heidelberg, Germany
*Address for Correspondence: Jan Jacobs, M.D., Department of General, Visceral, Trauma and Thoracic Surgery, Hospital of Ludwigshafen, Bremserstr. 79, 67063 Ludwigshafen am Rhein, Germany, Tel: +49 (0)621 503-3150; Fax: +49 (0) 621 503-3184; E-mail: cha@klilu.de
Citation: Hirche Z, Hirche C, Kremer T, Kneser U, Willis S, et al. Phylloides Tumors of the Breast: A Case Series with Review of the Literature. J Surgery. 2015; S(2): 6.
Copyright © 2015 Hirche Z, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 2
Submission: 18 April 2015 | Accepted: 02 June 2015 | Published: 06 June 2015
Editors:Dr. Marlon A Guerrero, Assistant Professor of Surgery, University of Arizona, USADr. James A Warneke, Associate Professor of Surgery, University of Arizona, USA
Abstract
Introduction: Phylloides tumors (PT) represent a rare entity of fibroepithelial breast tumors. The incidence ranges between 0.3-1% of all breast tumors. PT tend to have a high local recurrence rate, ranging between 28-46% after local excision. Due to their very low incidence, the available evidence is limited. A recent review of the literature accompanied by a presentation of routine and extraordinary PT cases from our hospital focuses on an update for treatment and oncological outcome of this rare entity.Patient and method: A Medline analysis was performed to extract recent literature on PT. The review of the literature was matched with a retrospective analysis of all PT cases treated between 2003 and 2012 in our hospital. The analysis included PT characteristics and histology, surgical procedures and an outcome evaluation. A case demonstration was included to visualize an extreme rare and challenging, infiltrating PT.
Results: In our study, 2 out of 9 patients suffered from benign PT (BPT) (22.2%), one from borderline PT (BLPT) (11.1%) and six from malignant PT (MPT) (66.7%). The tumor size ranged from 2.5 to 4 cm for BPT, 1.5 cm for BPLT and 4.5 to 23 cm for MPT. Six patients underwent local excision, while 2 patients were treated with mastectomy and one patient required individualized surgery by a multi surgical approach with radical tumor resection and plastic surgical reconstruction. This complex case is demonstrated separately. All nine patients underwent surgery with disease-free margins (100%). The review of the literature revealed no existing guidelines for the treatment of PT, thus the therapeutical management remains without standardization. There is consensus, that surgery is the 1st line therapy of PT and ranges from local excision, mastectomy to radical, wide resections. The inalienable factor for prognosis appears to be a margin-free-resection > 1 cm.
Conclusion: Only in rare cases, complex and individualized, multi surgical approaches with plastic surgical reconstruction are necessary for PT. While most cases are seen as MPT, even BPT and BLPT tend to malignant transformation, local recurrence and systemic spread. Treatment requires an individual approach due to the varying biological features and tumor size. From literature perspective, diseasefree specimen margins are the prime principle for all PT subtypes to achieve optimal oncological treatment.
Keywords:
Phylloides tumor; Cystosarcoma phylloides; MPT, BPT, BLPT; Chest wall reconstructionBackground
Phylloides tumors (PT) – also known as Cystosarcoma phylloidesare rare neoplasms of the breast [1]. They were initially described by Müller in 1838 [2]. In 1982, the WHO altered the original description “cystosarcoma phylloides” into the term “phylloides tumor” which accounts for the varying biological characteristics. Predominantly, women at age ranging between 35-45 years develop PT [3]. Among all breast cancer entities, the incidence is <1% [1]. As a consequence of its low incidence worldwide, diagnosis, treatment and prognosis of this rare entity is non-standardized and based on limited evidence [4].From clinical perspective, PT prone to grow rapidly, and distant metastases are rare even in large tumours which has been reported in 0-20%. Haematogenous metastatic spread involves the lung (66%), bones (28%) and the liver in up to 15% [1,5-7]. The incidence of lymphatic dissemination to axillary lymph nodes is 1.5% [5,8]. After surgical or multimodal treatment, the mean 5-year survival rate is 90% [3].Histologically, PT originate from the intralobular stroma of the breast and are characterized by both epithelial and mesenchymal cells [8]. PT are classified analogue to Elston and Ellis as benign (BPT), borderline (BLPT), or malignant (MPT) [9]. The classification is based on histological evaluation of potential cellular atypia, anaplasia, the degree of mitotic activity and infiltration rate [5]. Interestingly, even BPT metastasize and tend to recur in up to 46% [10]. Generally, the primarily recommended therapy is the surgical approach and varies from local excision of BPT to radical, wide resection of MPT. Early diagnosis and oncological surgery with disease-free margins are parameters with a significant influence on the prognosis.The aim of this study was to provide an update on treatment paths and oncological outcome of the rare entity of PT by runninga retrospective analysis of PT treated in our institution and a review of the recent literature. Based on the results and the literature, we attempted to provide an up-to-date treatment protocol for PT.Patients and Methods
PatientsWe performed a retrospective analysis of patients between 2003 and 2012 (10 years), who were diagnosed with PT and underwent treatment at our institution. Medical records of these patients were reviewed and clinical characteristics retrieved, included gender, age, oncological features of PT including tumor size and tumor location, type of surgery, histological data regarding subtype of PT and diseasefree margins, survival rate, morbidity and mortality (Table 1).
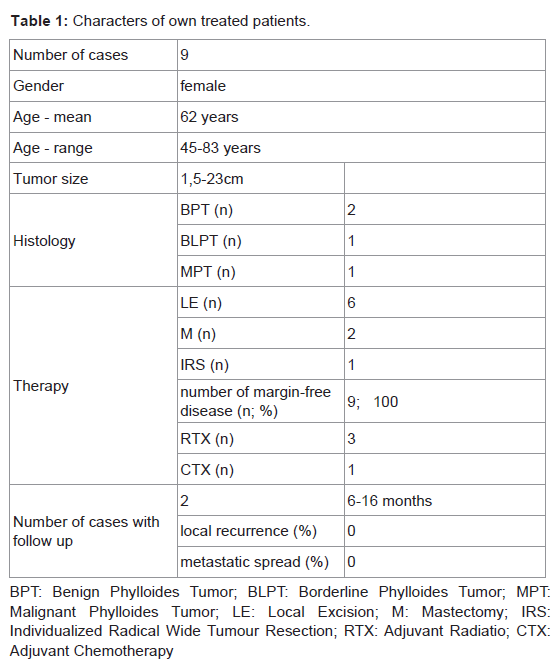
Table 1: Characters of own treated patients.
Literature review
We conducted a systematic literature research in Medline, using the terms “phylloides tumors”, “cystosarcoma phylloides” and “breast mass”.Analysis of each reference included objectification of the total number of included patients, local recurrence rate, rate of metastatic spread, surgical approach and application of adjuvant radiation or chemotherapy (Table 2). Some studies enabled separated evaluation of tumor subtype (BPT, BLPT and MPT) was possible. All further results from literature review are displayed in Table 2.
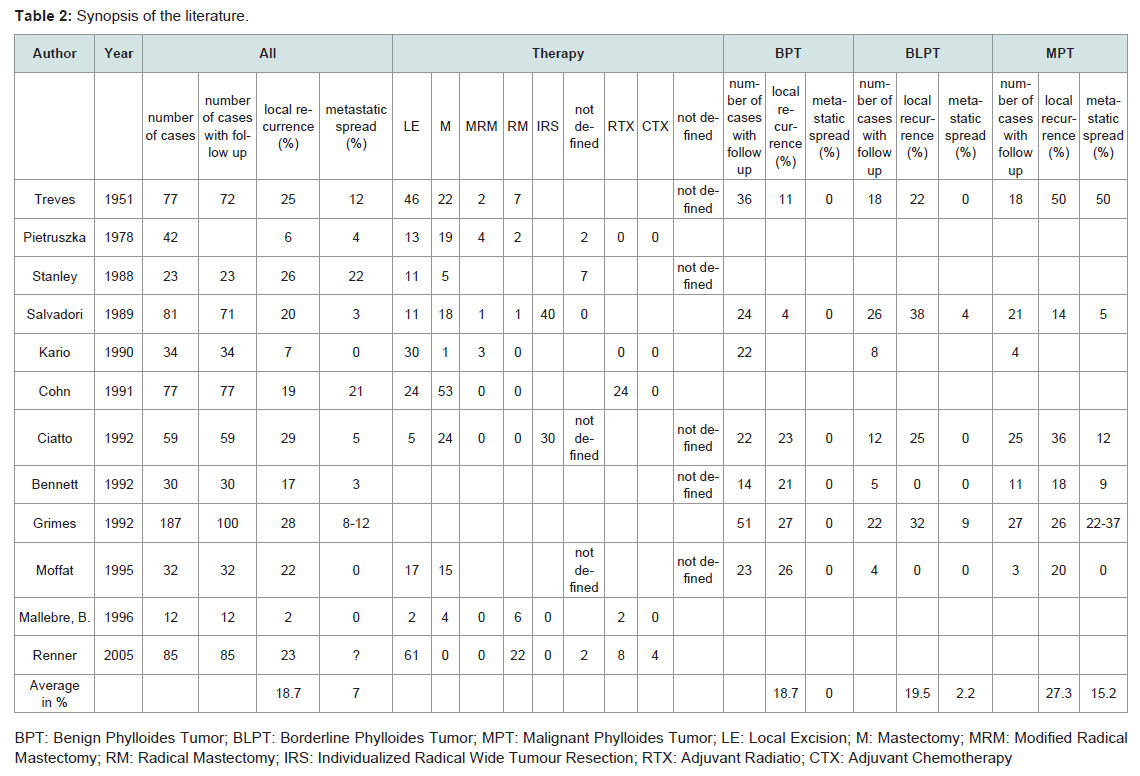
Table 2: Synopsis of the literature.
Results
Own dataRetrospective chart review revealed 9 eligible cases of female patients with PT treated between 2003 and 2013. The mean age was 62 years, ranging from 45-83 years. Histological evaluation revealed 2 out of 9 patients suffering from BPT (22.2%), one from BLPT (11.1%) and 6 from MPT (66.7%) (Table 1). The size of the tumors ranged from 2.5 to 4 cm for BPT, 1.5 cm for BPLT and 4.5 to 23 cm for MPT. All patients primarily received a surgical treatment under curative intention (Table 1). Six patients underwent a local excision, hereunder two cases with a BPT, one with a BLPT and 3 with a MPT histologically. Two patients, who suffered from MPT, underwent a mastectomy. The MPT patient with a diameter of 23 cm was a rare and complex case which required multi surgical management with individualized radical wide tumour resection by radical mastectomy and partial chest wall resection followed by reconstruction with alloplastic mesh, a regional transposition flap and mesh graft transplantation. This case is further summarized and displayed in Figures 1-4.

Figure 1: Tumor extend of a giant MPT before surgery (extent of 23 x 16 x 8.5 cm as a sturdy mass of the left breast).
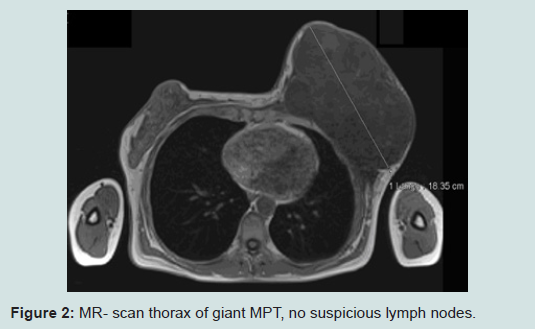
Figure 2: MR- scan thorax of giant MPT, no suspicious lymph nodes.
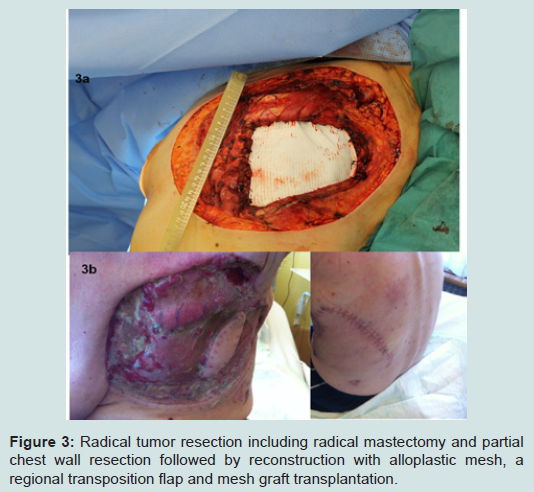
Figure 3: Radical tumor resection including radical mastectomy and partial chest wall resection followed by reconstruction with alloplastic mesh, a regional transposition flap and mesh graft transplantation.

Figure 4: 10 months later.
Discussion
Independent of their histopathological characteristics, PT requires sophisticated treatment strategies. Major challenges derive from large and bulky, fast growing PT, which have a high local recurrence rateexpected in 28-46% of cases [5]. Furthermore, individual tumor growth characteristics and dissemination cannot be predicted. In most cases, a curative intention is affordable after complete surgical excision with disease-free margins of the specimen [8].Surgery
Analysis of our data showed, that in all cases surgery was successfully completed with disease-free margins. Two BPT-, one BLPT- and three MPT-cases underwent local excision; two MPTcases underwent simple mastectomy. In one MPT-case, we performed an individualized radical wide tumour resection. We conclude that the surgical approach can be performed with regard to the tumor size and location. The choice of type of the surgical procedure did not primarily orientate on the histological subtype, but on the tumor extent. In three MPT-cases, we performed a local excision, because tumor size of 4.5-5.8 cm in relation to breast size was manageable. In all cases, specimen margins were disease-free.Although follow-up rate of 22.2% is unsatisfactory, we may conclude that the determining factor of prognosis is a margin-free resection.
Our findings are in agreement with the literature data: The recommend first line therapy is surgical excision, regardless of the benign or malignant character [14]. Usually, axillary lymph node dissection is not necessary for the treatment of PT [17,21]. Since lymphnode involvement is rare (in MPT 10%) [22], axillary dissection is only indicated, if suspicious nodes are detected (examination and imaging) [22]. Regarding the surgical management, the most important factor is complete removal of the tumor [17]. Patients should be treated by an individualized treatment concept. Tumor size, tumor location and extent as well as the size of the patient’s breasts have influence on decision-making. Bulky lesions may require a mastectomy, in some cases accompanied by partial or total thoracic wall resection. Small tumors can be locally excised with a wide cuff of tissue [14]. Removal of the pectoral fascia and/or muscle is not indicated, unless they are involved (imaging, intraoperative adhesions) or when resection margins are close [14]. A safety margin not less than 10 mm is recommended [1]. If margins >10 mm are attained, the local failure rate even for malignant lesions decreases under <20% [1,23]. As a consequence, an inadequate surgical excision negatively influences the outcome [24]. Some authors report, that incomplete excision appeared to be by far the most important determinant of recurrence [9]. In case of recurrence, PT is usually treated with secondary surgery [22]. Contrary to other benign or borderline neoplasms, especially BPT and BLPT have an unpredictable proliferative behaviour. BPT may lead to recurrent or metastatic disease [5]. They recur early and frequently [24]. Furthermore, recurrence of BPT can occasionally present with atypical transformation and may warrant the new diagnosis of MPT [24]. Thus Hajdu and co-workers indicated that even BPT should be excised with a generous portion of adjacent mammary tissue to prevent recurrence [24]. Overall, it has been suggested that all PT should be regarded as having a malignant potential. Moreover it is recommended that patients with borderline and benign PT have regular scheduled follow-ups.In literature, the adequacy of margins has never been subject of prospective, controlled and randomized trials. This issue should beinvestigated in further studies to achieve further evidence for PT.Most authors have advocated surgery to be the treatment of choice. Some have suggested to perform breast-conserving surgery (with disease-free margins) whenever possible [18]. Nevertheless, larger tumors and MPT have a higher risk of local recurrence [7,13,16,17]. Ciatto and co-workers showed a higher rate of local recurrence in MPT than in BPT with 36% vs. 23% [7]. Similarly results was shown by Treves and co-workers (50% vs. 11%) [13] and Salvadori and co-workers (24% vs. 4%) [16]. These studies suggest that huge malignant phylloides tumors should be primarily be treated with extended radical resection.
Our findings are in agreement with the literature data: The recommend first line therapy is surgical excision, regardless of the benign or malignant character [14]. Usually, axillary lymph node dissection is not necessary for the treatment of PT [17,21]. Since lymphnode involvement is rare (in MPT 10%) [22], axillary dissection is only indicated, if suspicious nodes are detected (examination and imaging) [22]. Regarding the surgical management, the most important factor is complete removal of the tumor [17]. Patients should be treated by an individualized treatment concept. Tumor size, tumor location and extent as well as the size of the patient’s breasts have influence on decision-making. Bulky lesions may require a mastectomy, in some cases accompanied by partial or total thoracic wall resection. Small tumors can be locally excised with a wide cuff of tissue [14]. Removal of the pectoral fascia and/or muscle is not indicated, unless they are involved (imaging, intraoperative adhesions) or when resection margins are close [14]. A safety margin not less than 10 mm is recommended [1]. If margins >10 mm are attained, the local failure rate even for malignant lesions decreases under <20% [1,23]. As a consequence, an inadequate surgical excision negatively influences the outcome [24]. Some authors report, that incomplete excision appeared to be by far the most important determinant of recurrence [9]. In case of recurrence, PT is usually treated with secondary surgery [22]. Contrary to other benign or borderline neoplasms, especially BPT and BLPT have an unpredictable proliferative behaviour. BPT may lead to recurrent or metastatic disease [5]. They recur early and frequently [24]. Furthermore, recurrence of BPT can occasionally present with atypical transformation and may warrant the new diagnosis of MPT [24]. Thus Hajdu and co-workers indicated that even BPT should be excised with a generous portion of adjacent mammary tissue to prevent recurrence [24]. Overall, it has been suggested that all PT should be regarded as having a malignant potential. Moreover it is recommended that patients with borderline and benign PT have regular scheduled follow-ups.In literature, the adequacy of margins has never been subject of prospective, controlled and randomized trials. This issue should beinvestigated in further studies to achieve further evidence for PT.Most authors have advocated surgery to be the treatment of choice. Some have suggested to perform breast-conserving surgery (with disease-free margins) whenever possible [18]. Nevertheless, larger tumors and MPT have a higher risk of local recurrence [7,13,16,17]. Ciatto and co-workers showed a higher rate of local recurrence in MPT than in BPT with 36% vs. 23% [7]. Similarly results was shown by Treves and co-workers (50% vs. 11%) [13] and Salvadori and co-workers (24% vs. 4%) [16]. These studies suggest that huge malignant phylloides tumors should be primarily be treated with extended radical resection.
Radiotherapy
In our cohort, two patients received adjuvant radiotherapy because of safety margins barely < 1 cm.Adjuvant radiotherapy is indicated to improve survival and reduce local recurrence. Nevertheless, the role of adjuvant adiotherapy remains controversial. There are only a few studies addressing radiotherapy in PT, which have a very limited statistical power due to their very small sample sizes. August and co-workers postulated adjuvant radiotherapy to improve the disease-free survival [23]. Some authors recommended the regular use of postoperative radiotherapy in malignant PT. There was no significant difference in terms of distant metastasis-free survival between patients who received radiation therapy and those who did not [18]. Stranzl and co-workers recommended that postoperative local radiotherapy was indicated for BLPT and MPT, if there are any adverse factors, such as large preoperative tumors and close or uncertain resection margins. At present, radiotherapy is occasionally applied in patients with recurrent disease (and in those with symptomatic metastases) [8,25,26].Based on the literature review and our own experience, we recommend radiotherapy in cases of disease-free specimen margins <1 cm. After secondary surgery due to local recurrence, adjuvant radiotherapy may be indicated based on an individual concept. Also if a secondary surgery is not possible, a radiotherapy may be a good alternative option. In case of BLPT and MPT, the high incidence of local recurrence should be taken into consideration, and adjuvant radiotherapy offered to the patient aiming at improved local control.
Chemotherapy
Malignant PT may give rise to haematogenous metastases in approximately 22% of cases [7,9]. Radical wide resection may reduce the risk of local recurrence, but has not been shown to be effective in preventing metastatic spread [9]. In case of chemotherapy, Ifosfamid has been applied on an individual therapeutic basis, but with scant effect [11]. In addition, hormonal therapy only showed a slight response [11]. Furthermore, adjuvant chemotherapy with doxorubicin and dacarbazine does not affect patient survival [27]. Reinfuss and co-workers, as well as Schwentner and co-workers reported the role of chemotherapy still to be defined; nowadays, there are several regimens mainly based on anthracyclines or ifosfamide/cyclophosphamide [26]. Altogether, there is no clear indication for adjuvant chemotherapy for patients with PT, and chemotherapy should only be performed under surveillance conditions.
Conclusion
Only in rare cases, complex and individualized, multi surgical approaches with plastic surgical reconstruction are necessary for PT. While most cases are seen as MPT, even BPT and BLPT tend to malignant transformation, local recurrence and systemic spread. Treatment requires an individual approach due to the varying biological features and tumor size. From literature perspective, disease-free specimen margins are the prime principle for all PT subtypes to achieve optimal oncological treatment.References
- Arcuri MF, Del Rio P, Martella EM, Bezer L, Sianesi M (2007) Giant malignant phylloides tumor: case report. G Chir 28: 251-252.
- Mangi AA, Smith BL, Gadd MA, Tanabe KK, Ott MJ, et al. (1999) Surgical management of phyllodes tumors. Arch Surg 134: 487-492.
- Kapiris I, Nasiri N, A'Hern R, Healy V, Gui GP (2001) Outcome and predictive factors of local recurrence and distant metastases following primary surgical treatment of high-grade malignant phyllodes tumours of the breast. Eur J Surg Oncol 27: 723-730.
- Palmer ML, De Risi DC, Pelikan A, Patel J, Nemoto T, et al. (1990) Treatment options and recurrence potential for cystosarcoma phyllodes. Surg Gynecol Obstet 170: 193-196.
- Bennett IC, Khan A, De Freitas R, Chaudary MA, Millis RR (1992) Phyllodes tumours: a clinicopathological review of 30 cases. Aust N Z J Surg 62: 628-633.
- Kessinger A, Foley JF, Lemon HM, Miller DM (1972) Metastatic cystosarcoma phyllodes: a case report and review of the literature. J Surg Oncol 4: 131-147.
- Ciatto S, Bonardi R, Cataliotti L, Cardona G (1992) Sarcomas of the breast: a multicenter series of 70 cases. Neoplasma 39: 375-379.
- Eich PD, Diederich S, Eich HT, Micke O, Wagner W (2000) Diagnostic radiation oncology: malignant cystosarcoma phylloides. Strahlenther Onkol 176: 192-195.
- Moffat CJ, Pinder SE, Dixon AR, Elston CW, Blamey RW, et al. (1995) Phyllodes tumours of the breast: a clinicopathological review of thirty-two cases. Histopathology 27: 205-218.
- Mundhenke C, Schem C (2013) Borderline cases of mamma carcinoma. Der Gynäkologe 42: 705-710.
- Renner K, Holzer B, Minai-Pour M, Hofmann M, Reiner-Concin A, et al. (2005) Phyllodes tumours of the breast. Eur Surg 37: 327-330.
- Barth RJ Jr, Wells WA, Mitchell SE, Cole BF (2009) A prospective, multi-institutional study of adjuvant radiotherapy after resection of malignant phyllodes tumors. Ann Surg Oncol 16: 2288-2294.
- Treves N, Sunderland DA (1951) Cystosarcoma phyllodes of the breast: a malignant and a benign tumor; a clinicopathological study of seventy-seven cases. Cancer 4: 1286-1332.
- Pietruszka M, Barnes L (1978) Cystosarcoma phyllodes: a clinicopathologic analysis of 42 cases. Cancer 41: 1974-1983
- Stanley MW, Tani EM, Rutqvist LE, Skoog L (1989) Cystosarcoma phyllodes of the breast: a cytologic and clinicopathologic study of 23 cases. Diagn Cytopathol 5: 29-34.
- Salvadori B, Cusumano F, Del Bo R, Delledonne V, Grassi M, et al. (1989) Surgical treatment of phyllodes tumors of the breast. Cancer 63: 2532-2536.
- Kario K, Maeda S, Mizuno Y, Makino Y, Tankawa H, et al. (1990) Phyllodes tumor of the breast: a clinicopathologic study of 34 cases. J Surg Oncol 45: 46-51.
- Cohn-Cedermark G, Rutqvist LE, Rosendahl I, Silfversward C (1991) Prognostic factors in cystosarcoma phyllodes. A clinicopathologic study of 77 patients. Cancer 68: 2017-2022.
- Grimes MM (1992) Cystosarcoma phyllodes of the breast: histologic features, flow cytometric analysis, and clinical correlations. Mod Pathol 5: 232-239.
- Mallebré B, Ebert A, Perez-Cantó A, Hopp H, Opril F, et al. (1996) Cystosarcoma phylloides of the breast. A retrospective analysis of 12 cases. Geburtshilfe Frauenheilkd 56: 35-40.
- Rossi M, Finucci G, Cascini F, Bianchini M, Tassinari G (1992) Phyllodes tumor of the breast. Minerva Chir 47: 1047-1052.
- Khurshid A, Kayani N, Bhurgri Y (2006) Phylloides tumors in adolescent girls and young women in Pakistan. Asian Pac J Cancer Prev 7: 563-566.
- August DA, Kearney T (2000) Cystosarcoma phyllodes: mastectomy, lumpectomy, or lumpectomy plus irradiation. Surg Oncol 9: 49-52.
- Hajdu SI, Espinosa MH, Robbins GF (1976) Recurrent cystosarcoma phyllodes: a clinicopathologic study of 32 cases. Cancer 38: 1402-1406.
- Zurrida S, Bartoli C, Galimberti V, Squicciarini P, Delledonne V, et al. (1992) Which therapy for unexpected phyllode tumour of the breast? Eur J Cancer 28: 654-657.
- Reinfuss M, Mitus J, Stelmach A (1995) Phyllodes tumor of the breast. Strahlenther Onkol 171: 5-11.
- Morales-Vásquez F, Gonzalez-Angulo AM, Broglio K, Lopez-Basave HN, Gallardo D, et al. (2007) Adjuvant chemotherapy with doxorubicin and dacarbazine has no effect in recurrence-free survival of malignant phyllodes tumors of the breast. Breast J 13: 551-556.