
Special Issue: Plastic and Reconstructive SurgeryCase Report
*Address for Correspondence: Reiner Josef Wirbel, Department of Trauma, Hand and Reconstructive Surgery, Verbundkrankenhaus Bernkastel-Wittlich, Koblenzer Str. 91, D-54516 Wittlich, Germany, Tel: 0043-6571-1532310; Fax: 0043-6571-1532390; E-mail: reiner.wirbel@web.de
Citation: Wirbel RJ, Weber S, Mutschler W. The Need for Reconstructive Surgery in Soft Tissue Sarcomas - Long-Term Functional Results and Quality of Life. J Surgery. 2015; S(1): 10.
Copyright © 2015 Wirbel RJ, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 09 March 2015 | Accepted: 27 March 2015 | Published: 04 April 2015
Editor: Dr. Abdou Mohammed Abd Allah Darwish, Head of the Department of Plastic & Reconstructive Surgery Minia University, Egypt


 Amputations had to be performed in 20 patients (9.8%): hemipelvectomy in 6 cases, the lower extremity in 9, and the upper extremity in 5 cases, respectively.
Amputations had to be performed in 20 patients (9.8%): hemipelvectomy in 6 cases, the lower extremity in 9, and the upper extremity in 5 cases, respectively.
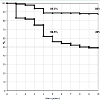
 The overall survival was significantly dependent upon the tumour stage after 5 years as well as after 10 years. The survival probability of 56.5% after 5 years decreased in patients with high-grade sarcomas to 49% after 10 years, whereas the reduction of the survival probability during this period was insignificant in patients with low-grade sarcomas (89.5% to 88%). Stage-III-tumours and intralesional resections were not considered.
The overall survival was significantly dependent upon the tumour stage after 5 years as well as after 10 years. The survival probability of 56.5% after 5 years decreased in patients with high-grade sarcomas to 49% after 10 years, whereas the reduction of the survival probability during this period was insignificant in patients with low-grade sarcomas (89.5% to 88%). Stage-III-tumours and intralesional resections were not considered.
 The best results were found in the category of function, and in the category of walking ability for the patients underwent tumour resection of the lower extremity. Only 3 out of the 27 patients of the lower extremity group needed walking frames.
The best results were found in the category of function, and in the category of walking ability for the patients underwent tumour resection of the lower extremity. Only 3 out of the 27 patients of the lower extremity group needed walking frames.
 Considering the symptoms-scales, the highest values were seen in the category “pain”, followed by the categories “fatigue” and “financial difficulties”.
Considering the symptoms-scales, the highest values were seen in the category “pain”, followed by the categories “fatigue” and “financial difficulties”.
The Need for Reconstructive Surgery in Soft Tissue Sarcomas - Long-Term Functional Results and Quality of Life
Reiner Josef Wirbel1*, Steffen Weber2 and Wolf Mutschler3
- 1Department of Trauma, Hand and Reconstructive Surgery, Verbundkrankenhaus Bernkastel-Wittlich, Wittlich, Germany
- 2Department of Trauma, Hand and Reconstructive Surgery, University Hospital of Saarland, Homburg-Saar, Germany
- 3Department of Surgery, Ludwig-Maximilians-Universität, München, Germany
*Address for Correspondence: Reiner Josef Wirbel, Department of Trauma, Hand and Reconstructive Surgery, Verbundkrankenhaus Bernkastel-Wittlich, Koblenzer Str. 91, D-54516 Wittlich, Germany, Tel: 0043-6571-1532310; Fax: 0043-6571-1532390; E-mail: reiner.wirbel@web.de
Citation: Wirbel RJ, Weber S, Mutschler W. The Need for Reconstructive Surgery in Soft Tissue Sarcomas - Long-Term Functional Results and Quality of Life. J Surgery. 2015; S(1): 10.
Copyright © 2015 Wirbel RJ, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Special Issue: 1
Submission: 09 March 2015 | Accepted: 27 March 2015 | Published: 04 April 2015
Editor: Dr. Abdou Mohammed Abd Allah Darwish, Head of the Department of Plastic & Reconstructive Surgery Minia University, Egypt
Abstract
The defect after resection of soft tissue sarcomas (STS) often requires reconstructive surgical procedures mostly allowing limb salvage. The prognosis of STS is mainly dependent on the tumour stage. Limited information exists about the long-term outcome and the influence of reconstructive surgery on the functional outcome and the quality of life.From 1993 until 2009, 203 patients (120 men, 83 women, mean age 52 years) with soft tissue sarcomas were treated surgically. The necessary reconstructive surgical procedures were analysed. To get information about the long-term outcome, 86 patients (51 men, 35 women) treated between 1993 and 1999 (follow-up > 10 years) were analyzed. The oncological outcome (local recurrences, metastases, overall survival) of 30 stage I-, 52 stage II- and 4 stage III-tumours was determined. Functional outcome and quality of life of the survivors were measured using the MSTS-criteria and the EORTC-QLQ-C-30 questionnaire after a mean follow-up of 144 months.
Different reconstructive procedures were necessary in 64 out of the 203 cases: 17 simple mesh graft, 32 muscle flaps, 3 tendon transfers, 8 vascular grafts and 4 bony reconstructions. The long-term survival was mainly influenced by the tumour stage. Survival rates of the stage II tumours were 56.5% and 49% after 5 and 10 years.
Thirty-six patients of the long-term follow-up group were dead after 10 years: 29 of their malignancy and 6 of other diseases.
The 50 long-term survivors presented good results for MSTS (mean score 82.4) and EORTC-QLQ-C-30 (mean score 79.8), the results were independent on the need of reconstructive surgery.
Concluding, different reconstructive surgical procedures can be necessary to close the defect after adequate resection of STS. The long-term functional results and the quality of life are not dependent on the procedure performed. Therefore, oncological and not functional aspects have to determine the extent of the adequate surgery.
Keywords
Reconstructive surgery; Quality of life; Soft tissue sarcoma; Long-termIntroduction
Soft tissue sarcomas represent a heterotopic group of tumours of mesenchymal origin which can be divided into low-grade and high-grade tumours by histo-morphologic criteria and by the clinical course.Beside the radiotherapy and the chemotherapy, the surgical therapy is the most important part of the multimodal treatment concept. However, considering the prognosis of patients with soft tissue sarcomas there remains the question of the adequate surgical treatment.
Several studies have shown, that the functional results are worse after amputation compared with those achieved with limb salvage procedures, but the quality of life is considered to be not dependent upon the surgical technique performed [1-7].
However, there remains the dilemma between the adequate surgery, i.e. the oncological and radical extent of the procedure, and the prevention of a serious loss of function, especially in soft tissue sarcomas localized in the extremities.
To close the defect after adequate resection reconstructive surgical procedures can be necessary. It is reported to be indicated in up to 50-80% of all cases [8,9]. There exist no detailed study about the influence of the need of reconstructive surgical procedures and the achieved function and quality of life.
Most of the studies of patients with soft tissue sarcomas have a limited follow-up of five years. Studies with long-term results of functional and oncological outcome and of the obtained quality of life are rare.
We like to focus on the long-term outcome by the presented retrospective study. The presented study has two primary goals: (1) to analyze the significance of surgery, especially the need for reconstructive procedures maybe compromising the functional outcome, and (2) to demonstrate the long-term (i.e. more than 10 years) oncological and functional results which can be expected in patients with soft tissue sarcomas.
Patients and Methods
PatientsA total of 203 patients with soft tissue sarcoma located at the trunk or the extremities were treated surgically in our depeartment from January 1993 to December 2009.
The necessity for reconstructive surgical procedure and the type of the procedures were analyzed.
The most frequent tumours were the malignant fibrous histiocytoma (n=61, 30.2%), the liposarcoma (n=45; 22%) and the leiomyosarcoma (n=28; 13.9%). Fibrosarcomas were seen in 19 cases (9.3%), rhabdomyosarcomas in 16 cases (8.1%), and synovialsarcomas in 13 cases (6.9%). There were 5 angiosarcomas, 5 malignant schwannomas, and 11 other tumour entities.
Concerning to the classification of Enneking [10] there were 71 (34.8%) low-grade (stage I) and 123 (60.4%) high-grade (stage II) tumours. In 9 cases distant metastases had to be observed (stage III).
To get informations about the long-term prognosis, patients with a minimum follow-up of 10 years or more (i.e. treated between 1993 and 1999) were selected and included in the study for oncological and functional evaluation.
In this group, there were 86 patients (51 men, 35 women) with an average age of 50.5 years (range, 16-86 years) at the date of surgery. There were 30 low-grade (stage I), 52 high-grade (stage II) tumours; in 4 cases there were distant metastases (stage III).
In 51.1% of the cases the tumour was localized in the lower extremity (n=44). In 26 cases (30.2%) the tumour originates from the upper extremity, and in 16 cases (18.7%) from the trunk, respectively.
Fifteen patients (17.4%) were presented with a local recurrence with a median interval of 23.6 months (range, 1 to 132 months) to the primary surgical procedure. In this group, there were 4 stage-I tumours, and 11 stage-II tumours. It was the first local recurrnce in 7 cases, two patients were admitted with a second local recurrence, three with the third, and three even with additional local recurrences, respectively.
All patients were informed that their data would be submitted for publication, and gave their consent.
Methods
Oncological follow-up care: All patients were regularly seen at the postoperative follow-up care. The demographic data were collected. The complications and the adjuvant therapies were also analyzed. The survival rate and the occurrence of local recurrence and metastases were determined. The survival probability was estimated by the method of Kaplan and Meier [11]. The achieved surgical margin [12], the tumour stage and the tumour volume were analyzed as prognostic factors for the incidence of local recurrence and/or metastases.
Function and quality of life: The performed surgical procedures (limb salvage procedure versus amputation) and the need for plasticreconstructive surgical techniques were analyzed and correlated with the achieved function and quality of life.
All survivors were examined at the last clinical follow-up in January 2010. The functional results were rated according to the MSTS-criteria [13]. The system includes the six following categories: pain, function of the affected joint, emotional acceptance, and for the lower extremity: supports, walking ability, and gait analysis, and for the upper extremity: hand positioning, manual dexterity, and lifting ability. A maximum of five points for each factor produces the maximum score of 30 points. The total score is divided by 30, resulting in the functional evaluation rate. The rating was considered excellent if five of the six factors scored five points, independent of the score of the sixth factor. A good rating was recorded if five factorsscored three points or more, and the sixth factor two points or less. A fair rating was regarded if five of the six factors scored one point or more, and the sixth factor zero points. If two or more factors scored zero points, the rating was considered poor.
To determine the quality of life, the QoL-C30 (quality of life - core module 30) - questionnaire was used [14,15]. Tumour-specific symptoms and functional impairments are considered in this questionnaire. The 30 questionnaire-items concern three different categories: global health status, functional scales (physical-, role-, emotional-, cognitive-, and social-functioning), and different symptom scales (fatigue, nausea and vomiting, pain, dyspnoea, insomnia, appetite loss, constipation, diarrhoea, and financial difficulties).
The answers are valued using a special formula [14]. The results represent each scale and subscale by a percent aged score. A high score in the functional scales and in the global health status means a good quality of life, whereas a high score in the symptom scales indicates a poor result.
ANOVA was used for statistical analysis of the oncological longterm results. To compare sub-groups T-test and Wilcoxon-test were applied. A p-value less than 0.05 was considered significant.
Results
Surgical treatmentIn the 71 low-grade tumours, the surgical margins achieved were wide in 50 cases, and marginal in 21 cases. In the 123 high-grade tumours the margins were radical in 17, wide in 50, marginal in 45, and intralesional in 11 cases. In the 9 stage-III tumours there were 5 marignal and 3 wide margins, and one intralesional margin.
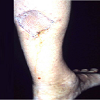
In 64 patients (31.5%) different plastic-reconstructive surgical procedures were necessary to close the soft tissue or bony defect produced by the resection of the tumour. In 17 cases simple mesh graft was sufficient (Figure 1); in 32 cases different local or free fasciocutaneous- or muscle-flaps (Figures 2 and 3) were needed. In three cases tendon transfer was necessary; vascular grafts (Figure 4) had to be performed in 8 cases. In 4 cases bony reconstructions had to be used (Figure 5) after additional resection of the involved bone or joint.

Figure 1: 34-year old man with a liposarcoma of the left-sided calf, simple closed of the defect by mesh graft.

Figure 2: 45-year old men with a fibrosarcoma at the left lateral ankle; a) latissimus free flap was necessary to close the defect, b) functional result showing only mild restriction of dorsal extension of the ankle joint 12 years later.

Figure 3: 46-year old man with a rhabdomyosarcoma of the right scapular area. Fasciocutaneous flap for closing the defect presented lateral wound healing problem after 2 weeks; it could be cured by renewed surgery
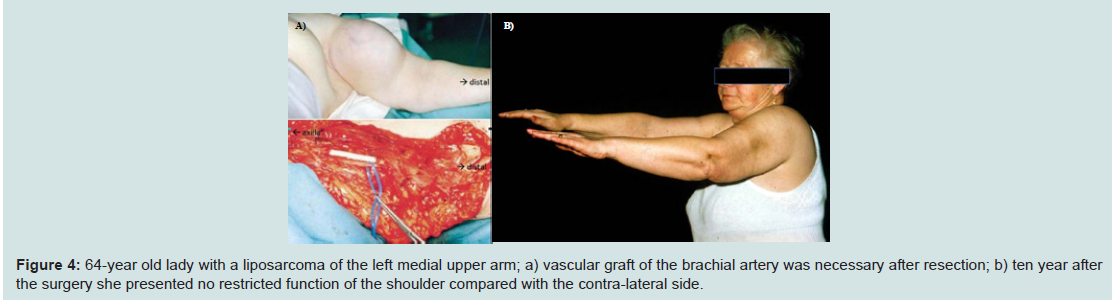
Figure 4: 64-year old lady with a liposarcoma of the left medial upper arm; a) vascular graft of the brachial artery was necessary after resection; b) ten year after the surgery she presented no restricted function of the shoulder compared with the contra-lateral side.
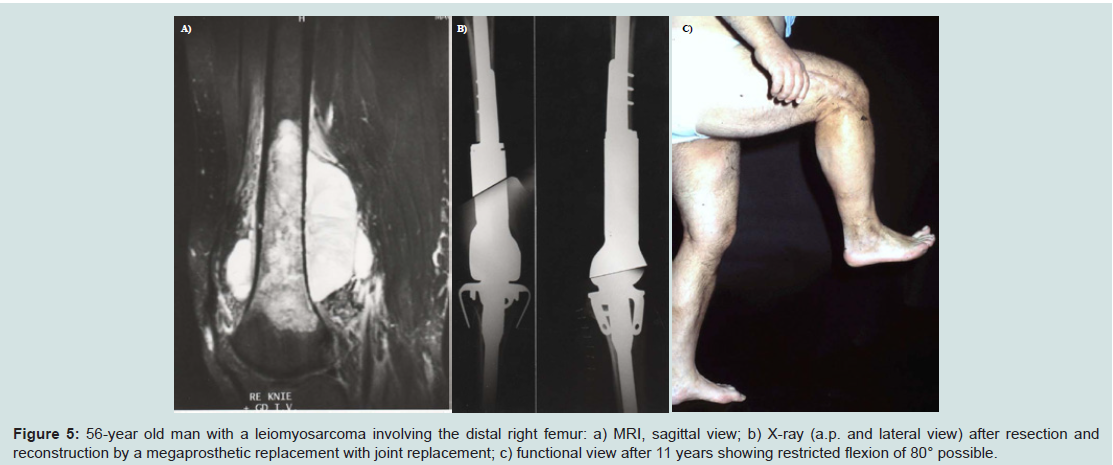
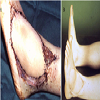
Figure 5: 56-year old man with a leiomyosarcoma involving the distal right femur: a) MRI, sagittal view; b) X-ray (a.p. and lateral view) after resection and reconstruction by a megaprosthetic replacement with joint replacement; c) functional view after 11 years showing restricted flexion of 80° possible.
The median tumour volume was 451 ml (range, 3-4800 ml). The stage-I tumours were smaller (386 ml) than the stage-II tumours (442 ml), but the difference was not significant.
In 35 patients (17.2%), 37 complications had to be observed. In most cases (n=30) there were wound healing problems requiring surgical revision in 20 out of these cases (Figure 3). All of these local complications could be cured. Further complications included four cases of a deep vein thrombosis, two cases of an osteonecrosis as the result of radiotherapy, and one case of a cerebrospinal fluid fistula requiring surgical closure.
Concerning the patient group with the long-term follow up (n = 86), reconstructive procedures were necessary in 9 of the 26 tumours (34.6%) located in the upper extremity and in 18 of the 44 tumours (40.9%) originating from the lower extremity. As expected, there were larger tumour volumes in these cases requiring reconstructive surgery measuring 620 ml on average (range, 250-4800 ml).
In this group, amputations had to be performed in 9 patients (10.4%): hemipelvectomy, the lower extremity, and the upper extremity, each in three times, respectively. Adjuvant therapies were performed in 43 patients out of these 86 patients with long-term follow up. Adjuvant radiotherapy was used in 23 cases, chemotherapy in 9 cases, and combined radio-chemotherapy in 11 cases. At the period of this study (i.e. from 1993 until 1999), adjuvant therapie were performed only in selected cases and in clinical trials. The indication for radiotherapy was usually seen in high-grade tumours and in large (i.e. > 5 cm) low-grade tumours. The indication for chemotherapy was proved only in clinical trials and studies without general guidline of recommendation.
Because of the restricted number of cases, and because of the individual indication for the adjuvant therapies in our series, relaible statistical evaluation of a potential benefit concerning the overall survival or the incidence of local recurrence was not feasible.
Oncological results in the patient group with long-term follow up:
At the date of evaluation 29 patients of the group with long-term follow up (n=86) died of their malignancy, and 7 patients died of other cases. The median survival time was 58 months (range, 26-74 months). The patients presenting with stage III tumours had a median survival time of 15.25 months. Local recurrences were observed in 13 patients (15.1%) after an average of 14.3 months (range, 4-47 months). Distant metastases were seen in 23 patients (26.7%) after an average of 11.7 months (range, 3-21 months). In most cases (n=21) there were pulmonary metastases.
The incidence of a local recurrence significantly depended upon the achieved surgical margin. The tumour volume had no influence. Concerning all tumour stages, local recurrences were significantly more frequent in cases of achieved marginal margin compared with those of wide or radical margin. These findings could be stated in both subgroups, (i.e. in the low-grade as well as in the high-grade tumours). The incidence of distant metastases was higher in highgrade tumours than in low-grade-tumours. But in both tumour subgroups, the incidence of distant metastases did not depend upon the surgical margin.
The 15 patients presented primarily with a local recurrence did not show worse oncological outcome. Most tumours (n=11) were high-grade tumours. The local recurrence could be cured in 10 out of these 15 patients.
Thirteen patients developed local recurrences. Ten of these cases occurred within the first two post-operative years. The local recurrences could be cured in four cases, twice by amputation, and twice by a renewed resection.
Distant metastases developed in 23 patients; 6 out of them were treated surgically. Only two patients could be cured, one by resection of a peripheral soft tissue metastasis, the other patient is considered as a complete responder after chemotherapy for 148 monts up to the date of evaluation. All other patients with distant metastases died of their disease.
The Kaplan-Meier long-term survival analyses in relation to the tumour stage and the achieved surgical margin are shown in Figures 6 and 7.
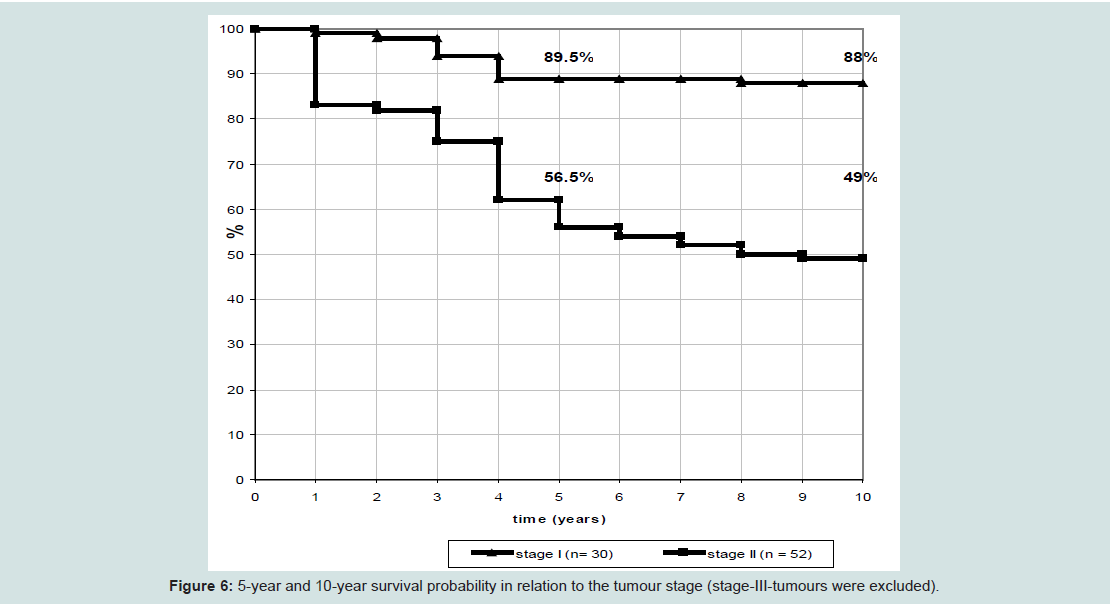
Figure 6: 5-year and 10-year survival probability in relation to the tumour stage (stage-III-tumours were excluded).
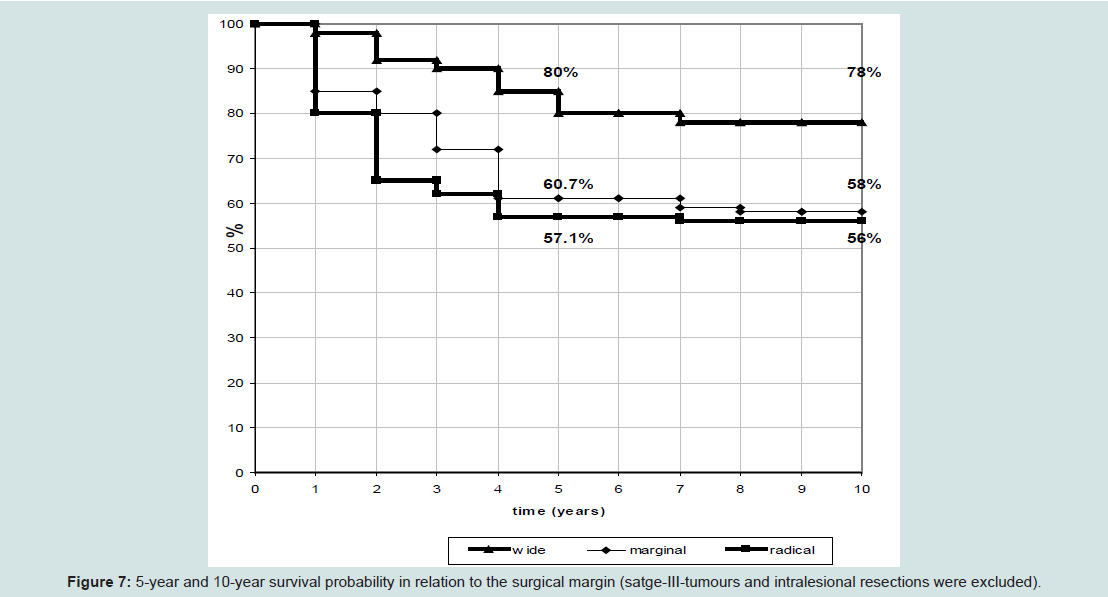
Figure 7: 5-year and 10-year survival probability in relation to the surgical margin (satge-III-tumours and intralesional resections were excluded).
Patients underwent wide resection showed a better prognosis than patients with marginal resection, but the difference was not significant. In both groups, there was a similiar reduction of the survival probability in the period of 5 years to 10 years postoperatively. The worse prognosis after radical resections can be explained by the fact that there were only high-grade tumours in this group.
There were also no differences in the 5-year and the 10-year survival rate concerning the tumour volume, the primary presentation with a local recurrence, or the fact of chemotherapy in high-grade sarcomas.
Functional results and quality of life in long-term survivors
Evaluations of function and of quality of life after an average follow-up of 12 years (range, 10 - 16 years) (i.e. 144 months (range, 120 - 192 months) were possible in 50 long-term survivors. There were 15 women and 35 men with a median age of 51.6 years (range, 28 - 81 years) at the date of evaluation. In 27 patients of the long-term survivors the tumour was localized in the lower extremity, in 15 cases in the upper extremity, and in 8 cases at the trunk.
The median MSTS-score was 82.4 % (range, 62-100 %). There were no significant differences concerning the patient’s age or sex and the localization of the tumour (Figures 4b and 5c). Thirty-eight of the 50 patients (76%) were free of pain.
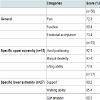
The 4 long-term surviving amputees showed marginal lower, but not significant different scores (median score 79.8%). The median scores of the categories pain, function, and emotional acceptance, as well as the specific scores for the upper and for the lower extremities are summarized in (Table 1). The specific scores showed marginal better values for the upper extremity, but there were no significant differences concerning the localization.
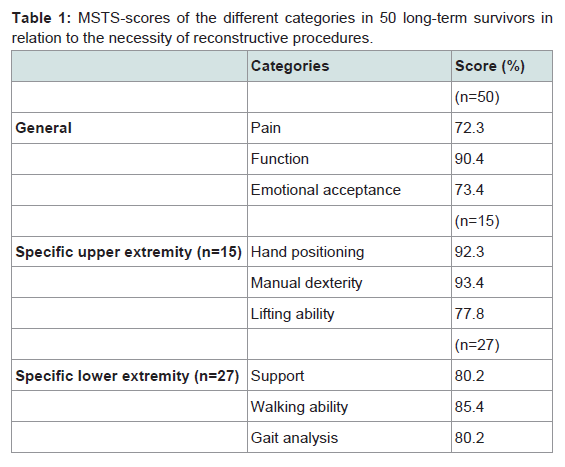
Table 1: MSTS-scores of the different categories in 50 long-term survivors inrelation to the necessity of reconstructive procedures.
The MSTS-scores of the patients underwent reconstructive surgical procedures did not differ from the scores of the patients without such procedures. The survivors treated primarily with adjuvant radiotherapy did also not present with worse results.
The results of the quality of life - QoL-C30-questionnaire are shown in Figure 8. There were no significant differences concerning patient’s age, sex, or localization of the tumour. The amputees also did not present with worse values. The best results were seen in the categories physical-, and cognitive-functioning. Thirty-two patients are retired, but only 4 of them (8%) were unable to work due to the tumour-disease. Fourteen patients (28%) stated a moderate or severe restriction of their daily activities. Six patients (12%) felt compromised in the category of social-functioning, and eight patients (16%) did so in the category of emotional-functioning.
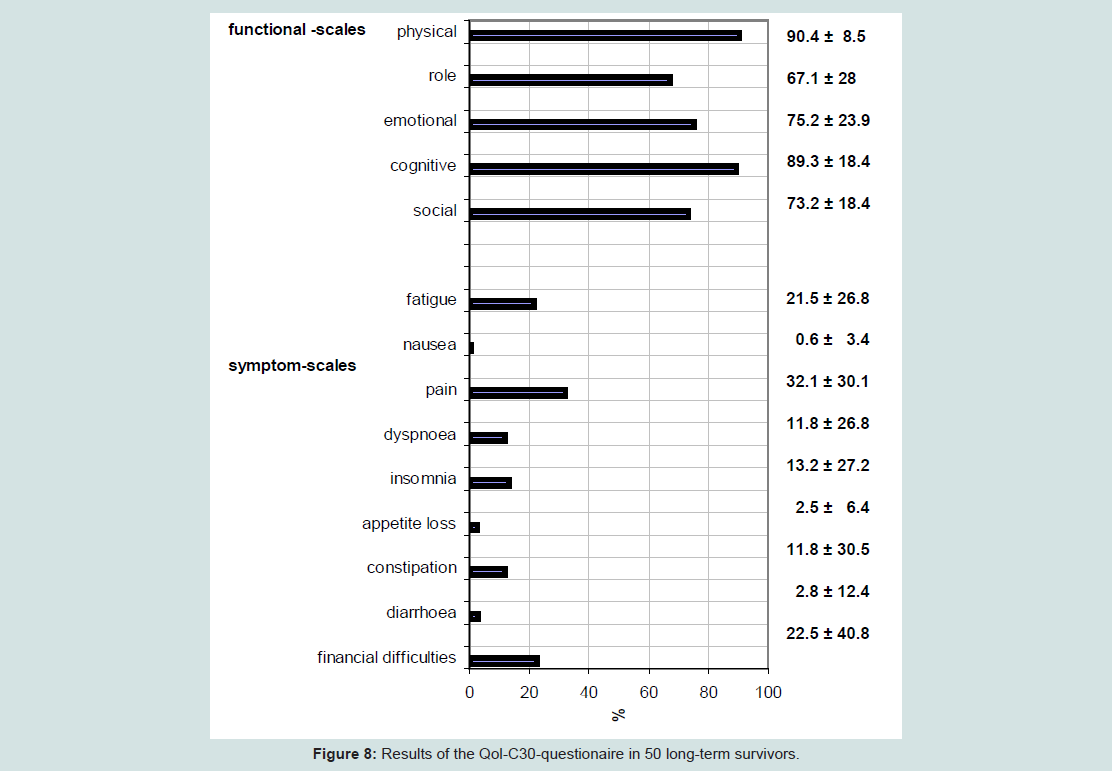
Figure 8: Results of the Qol-C30-questionaire in 50 long-term survivors.
Moderate pains were stated by 12 patients (24%); increased fatigue was reported by 11 patients (22%). Ten patients (20%) admitted financial problems due to their physical status, and due to their tumour treatment, respectively.
The symptoms-scales did also reveal no differences concerning patient’s age, sex, or localization of the tumour. The amputated patients presented also no worse values.
The global quality of life revealed a mean score of 72.8 (± 22.3) % without significant differences concerning localization of the tumour, patient’s age or sex, and concerning the performed surgical procedure(limb salving versus amputation) or the need for reconstructive procedures.
Discussion
Soft tissue sarcomas are very rare tumours accounting for less than 1% of all malignancies in the adult. Basically, they can be divided into low-grade and high-grade tumours by the means of histopathological criteria resulting in the surgical classification according to Enneking [10,12,16].The multimodal treatment concept includes surgery, radiotherapy, and chemotherapy. The two basic treatment goals are the local tumour control (i.e. the prevention of local recurrence) and the systemic tumour control (i.e. the prevention of distant metastases).
The significance of chemotherapy is seen in soft tissue sarcomas of the childhood, but in the adult there exist no clear guidelines. A possible benefit for the overall-survival has to be valued in further clinical trials and studies.
The significance of radiotherapy is meanwhile well defined for local tumour control [17,18]. In high-grade and in large (i.e. > 5 cm) low-grade tumours the recurrence-rate is significantly reduced. We can not make any relaibale statement about these adjuvant treatment modalities in our study, because at the time of our study period, the indication for radio- or chemotherapy was seen only in selected cases.
The predominant role of surgery in the treatment concept of soft tissue sarcomas is generally acknowledged [16,19]. But the extent of the surgical procedure is still a matter of discussion considering the prognosis of the different tumour stages and the possible loss of function. Wide resection has to be aspired for local tumour control 82 [4,16,17,19,20]. As shown in our series, the incidence of local recurrence is increased if only a marginal margin was achieved. The treatment of local recurrence is much more difficult, resulting in the loss of primarily preserved function in most of the cases.
By review of the literature, primary amputation is necessary in about 10% of the cases [2,4,7,19]. These reports agree with our findings (9.8%).
To close the defect after adequate resection different reconstructive surgical procedures can be necessary. Reconstructive surgery is reported to be indicated in up to 50-80% of cases [8,9]. In our series, reconstructive surgical procedures were necessary in 64 out of 203 patients (31.5%). The indication depends upon the localization of the tumour. To preserve the function and to avoid an amputation, reconstructive surgical procedures are more frequently indicated if the tumour is located peripherally [8,9]. The palette of the procedures procedures can range from simple mesh grafting to local, free muscle or fasciocutaneous flaps, to vascular grafting, to tendon transfers, and to extensive bony reconstructions. As expected and confirmed by our series, the need for plastic-reconstructive procedures is increased in large tumours, but we could not find any restriction in the long-term functional results.
The complication rate after resection of soft tissue sarcomas is reported to range from 25% to 30% [16-19], in most of the cases related to wound healing problems due to seromas or haematomas. The complication rate was 17.2% in our series. The large cavitations resulting from the resection of the tumour can fascilitate the occurrence of seromas. The indication for different muscle flaps can be seen in these cases. Planned vacuum sealing and second look procedures may help to minimize this problem.
In most cases, the long-term functional results after the resection of soft tissue sarcomas are described as good. In our series the mean MSTS-score revealed even 82.4 points. These findings correspond with the data of the literature [1-4,17,20,21]. Our results did not depend upon the patient’s age or sex, upon the tumour volume, or upon the localization of the tumour [22]. These findings disagree with the observations of Davis et al., who reported negative influence on the function by the patient’s age, and by the tumour volume [1]. In our series, the functional results were also not compromised neither by the need for reconstructive surgical procedures nor by the fact of adjuvant radiotherapy. But a reliable statement concerning these both factors maybe influencing the functional results is not feasible because of the limited number of patients.
The MSTS-score is the most common measuring instrument [13] of the function in patients underwent resection of a soft tissue sarcoma. But the function is not the only determinate for the quality of life [2,5-7,14,20,23].
The QoL-C-30-questionnaire has been established during the lastdecade to determine the quality of life in tumour patients [14,15]. As confirmed by our findings, about 10% to 30% of the patients report a restriction of daily activities, and/or of the social-functioning [3,5-7,14,21,23].
Using the MSTS criteria, many studies report a worse functional result in amputees compared with those who underwent limb salving procedures [4,17,18,21]. In our series the MSTS-score was also lower in amputated patients, but not significantly. The results of the QoLC30-questionnaire showed comparable values, in amputations and in limb salvage procedures, respectively. These findings were confirmed by other authors [5-7,17,21,23], demonstrating that quality of life is not only defined by the achieved function. As described by a recent study [23] the quality of life in tumour patients is mostly affected by social integration and by participation of life roles.
Thereby it is confirmed once more that oncological and not functional aspects have to influence the choice of the adequate surgical procedure (amputation versus limb salvage).
Beside the attained functional result every tumour therapy has to be measured primarily by the achieved oncological outcome. The overall-survival mostly depends upon the tumour stage. The 5-yearssurvival probabilities range from 50-60% in stage-II tumours up to 80-90% in stage-I tumours [16,19,21]. These reports are confirmed by our findings presenting survival rates of 89.5% in stage-I tumours, and 56.5% in stage-II tumours. Most studies reported an oncological follow-up of 5 years [2,16-18,20,23]. But we could demonstrate in our series that the survival probability will decrease furthermore; low-grade sarcomas showed an insignificant decrease of survival probability from 89.5% after 5 years to 88% after 10 years, but highgrade sarcomas from 56.5% after 5 years to 49% after 10 years, respectively.
There are some other prognostic factors in soft tissue sarcomas reported in the literature, such as tumour type, tumour volume, and localization [18,22]. We could not confirm these observations, maybe due to the limited number of patients.
The overall survival in our series only depended upon the tumour stage. Low-grade sarcomas were on average smaller than the highgrade sarcomas (386 ml versus 442 ml), but the difference was not significant. The thought can be suggested, that low-grade sarcomas were smaller in our series and therefore resectable more frequently with a wide margin. However, we could not find a statistical significance. The 5-year survival rate was 60.7%, when a marginal margin was achieved, and it was 80%, when a wide margin was feasible; the 10-year survival rate was 58% and 78%, respectively.
However, we agree with other authors [16,19], that the achieved surgical margin is the most important prognostic factor for local tumour control. The incidence of a local recurrence was significantly higher in tumours resected with a marginal margin compared with those resected with a wide margin. We observed significantly more local recurrences, when only a marginal margin was feasible.
Some studies demonstrated that the occurrence of local recurrence promotes the development of distant metastases resulting in a poor overall survival [2,21]. In our series, we saw 15 patients presented with a local recurrence without concomitant distant metastases. Ten of them could be cured, and we could not find a worse oncological outcome. But the small number of cases may not allow any statistical predication.
When distant metastases are detected, the treatment approach is palliative in most cases. There are predominantly pulmonary metastases. In our series only two out of 23 patients with metastases are still alive.
Conclusions
- Different reconstructive surgical procedures can be necessary to close the defect after adeqaute resection of a soft tissue sarcoma;- Long-term functional results and the quality of life are not influenced by the surgical procedure performed,
- The quality of life is not only influenced by the achived function,
- Therefore, oncological and not functional aspects have to determine the extent of the surgical procedure,
- The tumour stage mainly influences the overall survival, the surgical margin achieved is the most importatnt factor for local tumour control,
- Different reconstructive surgical procedures can be necessary
- In high-grade sarcomas the survival rate will drop even after 5 years,
- Long-term studies with prolonged follow-up will be helpful to define the exact oncological outcome.
References
- Davis AM, Devlin M, Griffin AM, Wunder JS, Bell RS (1999) Functional outcome in amputation versus limb sparing of patients with lower extremity sarcoma: a matched case-control study. Arch Phys Med Rehabil 80: 615-661.
- Keus RB, Rutgers EJ, Ho GH, Gortzak E, Albus-Lutter CE, et al. (1994) Limb-sparing therapy of extremity soft tissue sarcomas: treatment outcome and long-term functional results. Eur J Cancer 30A: 1459-1463.
- Parsons JA, Davis AM (2004) Rehabilitation and quality of life issues in patients with extremity soft tissue sarcomas. Curr Treat Options Oncol 5: 477-488.
- Robinson MH, Spruce L, Eeles R, Fryatt I, Harmer CL, et al. (1991) Limb function following conservation treatment of adult soft tissue sarcoma. Eur J Cancer 27: 1567-1574.
- Sugarbaker PH, Barofsky I, Rosenberg SA, Gianola FJ (1982) Quality of life assessment of patients in extremity sarcoma clinical trials. Surgery 9: 17-23.
- Weddington WW Jr, Segraves KB, Simon MA (1985) Psychological outcome of extremity sarcoma survivors undergoing amputation or limb salvage. J Clin Oncol 3: 1393-1399.
- Zahlten-Hinguranage A, Bernd L, Ewerbeck V, Sabo D (2004) Equal quality of life after limb-sparing or ablative surgery for lower extremity sarcomas. Br J Cancer 91: 1012-1014.
- Steinau HU, Ehrl H, Biemer E (1988) Reconstructive plastic surgery in soft tissue sarcoma of the extremities. Eur J Plast Surg 11: 99-108.
- Steinau HU, Hauser J, Farzaliyev F, Podleska L (2014) Long-term funczional results after sarcoma resection. Chirurg 85: 215-220.
- Enneking WF (1986) A system of staging musculoskeletal neoplasms. Clin Orthop Relat Res 204: 9-24.
- Kaplan E, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Stat Assoc 53: 457-481.
- Enneking WF, Spanier SS, Goddman MA (1980) A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res 153: 106-120.
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ (1993) A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res 286: 241-247.
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, et al. (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international trials in oncology. J Natl Cancer Inst 85: 365-376.
- Fayers PM, Machin D (2000) Quality of life: Assessment, analysis and interpretation. Chichester, USA: J. Wiley & Sons.
- Pisters PW, Leung DH, Woddruff JM, Shi W, Brennan MF (1996) Analysis of prognostic factors in 1041 patients with localized soft tissue sarcoma of the extremity. J Clin Oncol 14: 1679-1689.
- Bell RS, O`Sullivan B, Davis A, Langer F, Chummings B, et al. (1991) Functional outcome in patients treated with surgery and irradiation for soft tissue tumours. J Surg Oncol 48: 224-231.
- Lampert MH, Gerber LH, Glatstein E, Rosenberg SA, Danoff JV (1984) Soft tissue sarcoma: functional outcome after wide local excision and radiation therapy. Arch Phys Med Rehabil 65: 477-480.
- Lewis JJ, Leung D, Espat J, Woddruff JM, Brennan MF (2000) Effect of resection in extremity soft tissue sarcoma. Ann Surg 231: 655-663.
- Aksnes LH, Bauer HC, Jebsen NL, Folleras G, Allert C, et al. (2008) Limb-sparing surgery preserves more function than amputation: a Scandinavian sarcoma group study of 118 patients. J Bone Joint Surg Br 90: 786-794.
- Davidge K, Bell R, Ferguson P, Turcotte R, Wunder J, et al. (2009) Patient expectations for surgical outcome in extremity soft tissue sarcoma. J Surg Oncol 100: 375-381.
- Gerrand CH, Wunder JS, Kandel RA, O'Sullivan B, Catton CN, et al. (2004) The influence of anatomic location on functional outcome in lower-extremity soft-tissue sarcoma. Ann Surg Oncol 11: 476-482.
- Schreiber D, Bell RS, Wunder JS, O’Sullivan B, Turcotte R, et al. (2006) Evaluation function and health related quality of life in patients treated for extremity soft tissue sarcoma. Qual Life Res 15: 1439-1446.