
Journal of Surgery
Download PDF
Case Report
*Address for Correspondence: Angela Echeverria, MD, Department of Surgery, Division of Trauma/Critical Care/Emergency Surgery, University of Arizona College of Medicine, Arizona, USA, E-mail: aechev@email.arizona.edu
Citation: Echeverria A, Rhee P, Aman M, Friese R, Tang A. Delayed Cardiac Injury from Gradual Bullet Fragment Erosion into the Right Ventricle. J Surgery. 2013;1(1): 2.
Copyright © 2013 Echeverria A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 1, Issue: 1
Submission: 26 July 2013 | Accepted: 27 August 2013 | Published: 30 August 2013
Reviewed & Approved by: Dr. Dominique Shum-Tim, Department of Surgery, McGill University, Canada
Penetrating cardiac injuries are among the most lethal of all traumatic injuries, with many studies citing mortalities of 70-90% [1-3]. Such injuries account for a very small proportion of annual trauma admissions (0.1%) with most institutions reporting fewer than 10 cases per year [3]. This presents a challenge to trauma care providers in becoming adept at rapidly identifying and treating penetrating cardiac injuries. Moreover, in contrast to other injury mechanisms, survival from penetrating cardiac injuries has shown only modest improvement over the last several decades. Most importantly, a high index of clinical suspicion, rapid diagnosis, and expeditious surgical treatment yields the best chance of survival. Current understanding of this injury pattern is largely based on case series due to its rarity. This manuscript adds to the body of literature on penetrating cardiac injuries by detailing a 29-year-old male who experienced fullthickness right ventricular erosion from cardiac contraction against an abutting bullet fragment, a process that developed within three hours from the time of injury. We will describe the epidemiology and review the diagnosis and treatment of penetrating cardiac injuries with specific reference to our unusual case.
 The patient remained hemodynamically stable, therefore a CT scan was obtained to further evaluate the bullet trajectory (Figures 2 and 3). The CT scan identified a metallic fragment abutting the right ventricle without associated hemopericardium, multiple metallic fragments within the peritoneal cavity, as well as free air and peritoneal free fluid.
The patient remained hemodynamically stable, therefore a CT scan was obtained to further evaluate the bullet trajectory (Figures 2 and 3). The CT scan identified a metallic fragment abutting the right ventricle without associated hemopericardium, multiple metallic fragments within the peritoneal cavity, as well as free air and peritoneal free fluid.

 The patient underwent an emergent laparotomy at which time three destructive small bowel injuries were resected followed by primary hand-sewn anastomoses. The patient remained hemodynamically stable during the operation and required only two units of PRBCs. Due to the proximity of the bullet fragment to the heart and the concern for cardiac erosion through normal cardiac motion, the operating surgeon proceeded with a subxiphoid window with the intention of bullet removal. Upon entrance into the pericardium, there was an immediate release of large volume of pulsatile venous blood indicating the presence of a cardiac injury. A median sternotomy was quickly performed while applying digital pressure through the pericardial window to achieve temporary hemostasis. A 2 cm full-thickness right ventricle laceration was found to be actively bleeding with the 1.7 cm bullet fragment lodged against it. The RV laceration was repaired with a single pledgetted horizontal mattress suture of 2-O prolene.
The patient underwent an emergent laparotomy at which time three destructive small bowel injuries were resected followed by primary hand-sewn anastomoses. The patient remained hemodynamically stable during the operation and required only two units of PRBCs. Due to the proximity of the bullet fragment to the heart and the concern for cardiac erosion through normal cardiac motion, the operating surgeon proceeded with a subxiphoid window with the intention of bullet removal. Upon entrance into the pericardium, there was an immediate release of large volume of pulsatile venous blood indicating the presence of a cardiac injury. A median sternotomy was quickly performed while applying digital pressure through the pericardial window to achieve temporary hemostasis. A 2 cm full-thickness right ventricle laceration was found to be actively bleeding with the 1.7 cm bullet fragment lodged against it. The RV laceration was repaired with a single pledgetted horizontal mattress suture of 2-O prolene.
Delayed Cardiac Injury from Gradual Bullet Fragment Erosion into the Right Ventricle
Angela Echeverria*, Peter Rhee, Mustafa Aman, Randall Friese and Andrew Tang
- Department of Surgery, Division of Trauma/Critical Care/Emergency Surgery, University of Arizona College of Medicine, Arizona, USA
*Address for Correspondence: Angela Echeverria, MD, Department of Surgery, Division of Trauma/Critical Care/Emergency Surgery, University of Arizona College of Medicine, Arizona, USA, E-mail: aechev@email.arizona.edu
Citation: Echeverria A, Rhee P, Aman M, Friese R, Tang A. Delayed Cardiac Injury from Gradual Bullet Fragment Erosion into the Right Ventricle. J Surgery. 2013;1(1): 2.
Copyright © 2013 Echeverria A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Surgery | ISSN: 2332-4139 | Volume: 1, Issue: 1
Submission: 26 July 2013 | Accepted: 27 August 2013 | Published: 30 August 2013
Reviewed & Approved by: Dr. Dominique Shum-Tim, Department of Surgery, McGill University, Canada
Penetrating cardiac injuries are among the most lethal of all traumatic injuries, with many studies citing mortalities of 70-90% [1-3]. Such injuries account for a very small proportion of annual trauma admissions (0.1%) with most institutions reporting fewer than 10 cases per year [3]. This presents a challenge to trauma care providers in becoming adept at rapidly identifying and treating penetrating cardiac injuries. Moreover, in contrast to other injury mechanisms, survival from penetrating cardiac injuries has shown only modest improvement over the last several decades. Most importantly, a high index of clinical suspicion, rapid diagnosis, and expeditious surgical treatment yields the best chance of survival. Current understanding of this injury pattern is largely based on case series due to its rarity. This manuscript adds to the body of literature on penetrating cardiac injuries by detailing a 29-year-old male who experienced fullthickness right ventricular erosion from cardiac contraction against an abutting bullet fragment, a process that developed within three hours from the time of injury. We will describe the epidemiology and review the diagnosis and treatment of penetrating cardiac injuries with specific reference to our unusual case.
Case Presentation
A 29-year-old male was transported to our trauma center after sustaining multiple gunshot injuries to the right chest and abdomen. On presentation, his heart rate was 109, blood pressure 159/109 mmHg, and respiratory rate was 24 BPM. He was mildly short of breath and did not have peritonitis. The right anterior axillary GSW over the 4th intercostal space presented concerns for cardiac injury, however the cardiac ultrasound was negative for hemopericardium. A Focused Assessment with Sonography in Trauma (FAST) of the abdomen did not reveal intraabdominal free fluid. A chest X-ray revealed a 1.7 cm irregular metallic fragment adjacent to the right heart border and right pulmonary contusion with moderate hemothorax. A right thoracostomy tube was placed with 250 cc of bloody return (Figure 1).
Figure 1 Chest X-ray showing bullet fragment in pericardium.
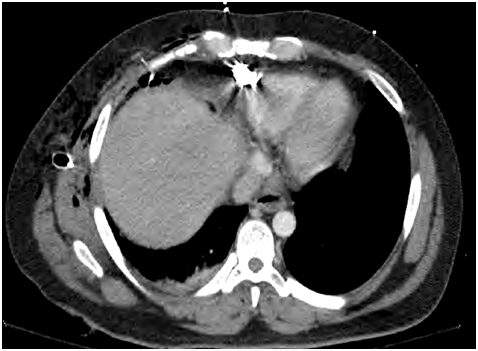
Figure 2 Axial CT showing bullet fragment anterior to right ventricle.
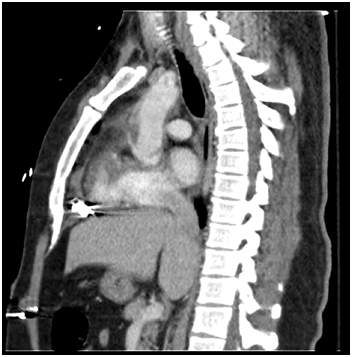
Figure 3 Sagittal CT showing bullet fragment in relation to heart.
The patient’s postoperative course was complicated by transfusion related acute lung injury (TRALI) requiring prolonged mechanical ventilation, temporary hemodialysis for self-limiting acute kidney injury that developed secondary to the TRALI induced severe physiologic compromise, and a right bronchopleural fistula repaired through a right thoracotomy. Following our institutional protocol for penetrating cardiac injuries, the patient underwent surveillance echocardiogram at two weeks post cardiorrhaphy which demonstrated an ejection fraction of 55%, normal wall motion and minimal tricuspid regurgitation. The patient has been followed for seven months since discharge and has been doing well with no residual physical limitations.
Discussion
Penetrating cardiac injuries are associated with an overall survival of 19-33% [4,5]. Survival rates for piercing cardiac injuries are 3 to 4 folds higher than survival rates for cardiac gunshot wounds. This has been attributed to the less destructive nature of piercing injuries and the overall less associated injury burden. Multiple retrospective series have documented prehospital death rates of 76-94% for cardiac gunshot wounds [3,6]. Time to definitive surgical care is the single most important predictor of survival for penetrating cardiac injuries. Pericardial tamponade has been theorized to confer a time-limited survival advantage by forestalling exsanguination [7]. However this is predicated on the expedient delivery of definitive surgical therapy as the length of this beneficial temporizing effect is unclear. Patients with untreated traumatic pericardial tamponade succumb to right atrial and ventricular compression as the pericardial pressure overwhelms the cardiac filling pressure resulting in loss of preload and subsequent cardiac arrest. In one of the largest series, it is estimated that 18% of deaths are potentially salvageable due to isolated cardiac wounds with tamponade [6]. The same study also identified higher survival rates for patients who had surgery within a 30-minute window.Patients with penetrating injuries to the cardiac box, bordered superiorly by the clavicles, inferiorly by the costal margins and laterally by the mid-clavicular lines are considered to have a cardiac injury until proven otherwise. Physical exam may reveal muffled heart sounds, distended neck veins, hypotension and an anxious patient who struggles to remain upright. Although Beck’s triad has been identified in up to 77% of patients with proven tamponade [3], these signs and symptoms alone are often not relied on for definitive diagnosis.
Bedside cardiac ultrasound is the diagnostic modality of choice for detecting pericardial tamponade. It is readily available, noninvasive, easy to perform, and repeatable. In a prospective multicenter study of 261 consecutive patients with suspected penetrating cardiac injuries, Rozycki found the cardiac ultrasound to be 100% sensitive and 97% specific for identifying cardiac tamponade. Immediate surgical repair, most of the time without cardiopulmonary bypass, is mandatory for patients with traumatic pericardial tamponade or hemorrhage. A resuscitative thoracotomy is the procedure of choice for hemodynamically unstable patients. For those hemodynamically stable patients with equivocal bedside cardiac ultrasound, further diagnostic options include surgical pericardial window, formal echocardiography or CT, although the latter studies are not routinely advocated in the traumatic setting in fear of patient sudden decompensation from hemodynamically significant pericardial tamponade or exsanguination.
Our patient presented a unique scenario in that he presented with hemodynamic stability and a deceivingly benign abdominal exam given his multiple thoracic and abdominal injuries. His cardiac ultrasound was negative for hemopericardium, which effectively ruled out a cardiac injury, this was further supported by the absence of hemopericardium on CT. While undergoing small bowel resections, the large metallic fragment lodged against the right ventricle caused a full thickness erosion and hemopericardium. The patient did not suffer the full effect of cardiac tamponade with hemodynamic compromise partially by fortuitous timing of the pericardial window initially performed for bullet removal.
There are multiple case reports in the literature on cardiac erosions from foreign bodies such as central lines or pace maker wires. However, this is the first report, to our knowledge, of a bullet erosion into a cardiac chamber due to the friction between the normal contractile motion of the heart and the adjacent bullet fragment. This report further attest to the importance of a thorough work up including routine chest X-ray, cardiac ultrasound, possibly CT scans in very selected cases to determine the presence of cardiac tamponade and to identify the relative relationship of the projectile to the heart. Most of all, the expedient diagnosis and treatment of cardiac injury is largely predicated on the treating physician’s “high index of suspicion” taking into account the patient’s mechanism of injury, anatomical location of injury and the patient’s physiology. Based on experience gained from this patient, we advocate removal of all foreign substances which abut the heart and present a risk for cardiac erosion through friction from cardiac motion.
References
- Buckman RF Jr, Badellino MM, Mauro LH, Asensio JA, Caputo C, et al. (1993) Penetrating cardiac wounds: prospective study of factors influencing initial resuscitation. J Trauma 34: 717-725.
- Kang N, Hsee L, Rizoli S, Alison P (2009) Penetrating cardiac injuries: overcoming the limits set by Nature. Injury 40: 919-927.
- Demetriades D, van der Veen BW (1983) Penetrating injuries of the heart: experience over two years in South Africa. J Trauma 23: 1034-1041.
- Rhee PM, Foy H, Kaufmann C, Areola C, Boyle E, et al. (1998) Penetrating cardiac injuries: a population-based study. J Trauma 45: 366-370.
- Asensio JA, Murray J, Demetriades D, Berne J, Cornwell E, et al. (1998) Penetrating cardiac injuries: a prospective study of variables predicting outcomes. J Am Coll Surg 186: 24-34.
- Campbell NC, Thomson SR, Muckart DJ, Meumann CM, Van Middelkoop I, et al. (1997) Review of 1198 cases of penetrating cardiac trauma. Br J Surg 84: 1737-1740.
- Moreno C, Moore EE, Majure JA, Hopeman AR (1986) Pericardial tamponade: a critical determinant for survival following penetrating cardiac wounds. J Trauma 26: 821-825.