Research Article Total Knee Arthroplasty with a Lateral Centre of Rotation Design Retained Native Knee Joint Kinematics: A Cadaveric Study under Simulated Muscle Loads
Karsten Engel1*, Katina Mira Fischer1, Gert-PeterBrüggemann1 and Christian Liebau2
- 1Institute of Biomechanics and Orthopedics, German Sport University Cologne, Germany
- 2Asklepios Harzklinik, Germany
*Address for Correspondence: Karsten Engel, Institute of Biomechanics and Orthopedics, German Sport University of Cologne, Am Sportpark Müngersdorf 6, 50933 Cologne, Germany, Tel: +49 (0) 221 - 4982 7630/+49; Fax: +49 (0) 221 - 4971598; E-mail:
k.engel@dshs-koeln.de Citation: Engel K, Fischer KM, Brüggemann GP, Liebau C. Total Knee Arthroplasty with a Lateral Centre of Rotation Design Retained Native Knee Joint Kinematics: A Cadaveric Study under Simulated Muscle Loads. J Orthopedics Rheumatol. 2016; 3(1): 6.
Copyright © 2016 Engel K, et al. This is an open access article distributed under the
Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 3, Issue: 1
Submission: 15 December 2015 | Accepted: 22 February 2016| Published: 27 February 2016
Abstract
Background: Since controversial results on the location of the centre of rotation in the native human knee joint exist, it is still unclear how the design of a total knee replacement should be in order to retain patients’ knee joint movement after Total knee Arthroplasty. Therefore, the aim of the present study was to determine individual native tibiofemoral joint kinematics as well as the centre of rotation and to investigate the influence of a total knee implant with a proposed lateral centre of rotation on the knee kinematics.
Materials and methods: The rotational and translational tibiofemoral joint kinematics of 9 cadaveric knees were captured under simulated muscle loads between 10° and 60° of flexion in a closed kinematic chain experiment. The entire foot and ankle complex was kept intact in order to maintain more realistic experimental conditions. The individual kinematics of the native joint condition were studied and compared to those after Total Knee Arthoplatsy.
Results: The rotational and translational kinematics showed quite a large variance, which can be explained with the individual anatomy. A medial centre of rotation was found in 8 specimens in the native joint, just one showed a lateral centre of rotation. After Total Knee Arthroplasty the centre of rotation changed to the lateral compartment in 5 specimens. Small differences were identified in the rotational kinematics between both experimental conditions, whereas the translation on both compartments and the centre of rotationshowed greater changes.
Conclusions: The investigated Total Knee Arthroplasty design had the ability to restore the individual joint kinematics, although the centre of rotation altered.
Introduction
The goal of a Total Knee Arthroplasty (TKA) is to relieve pain and ideally to regain the individual tibiofemoral joint kinematics. However, patients’ satisfaction after TKA ranges between 70% and 90% [
1-3], which might be associated with the different available implant designs and thus, in turn, with ongoing discussion on the kinematics of the native human tibiofemoral joint [
4-6]. In addition to cruciate substituting, cruciate retaining, mobile or fixed bearing designs, differentiation with regards to the location of the pivot, or more precisely with the centre of rotation (COR) of the knee joint, has to be taken into account. Knee implants with a medial COR design as well as implants with a lateral one can be found in several studies [
7-11]. The presence of the COR in the medial compartment was explained by the high congruence of the femoral epicondyle with the concave medial tibia surface and has been accepted for years [
12-14], whereas more recent studies obtained controversial results. During walking and dynamic activities a COR on the lateral compartment was found [
15-17], while during squats and kneeling a COR on the medial side was described [
18-20]. In contrast to this activity dependent motion pattern, it was found that the COR could be medial or lateral, depending not on the activity but on the individual person [
21].
An experimental investigation on the effect of a TKA with a lateral COR on the tibiofemoral joint kinematics and on the COR itself is still missing from the literature. Since these effects cannot be well studied in vivo, cadaveric studies have to be performed under simulated loading conditions. Varadarajan et al. showed that the captured kinematics in those experiments is comparable to those of in vivo studies [
22]. The authors’ demand for more physiological constraints has not been met to date, since in most experimental setups a simple mechanical joint replaces the ankle joint. Therefore, the aims of the present study were to determine (i) the individual native tibiofemoral joint kinematics including the COR and (ii) whether a total knee implant with a proposed lateral COR has the ability to restore the individual knee joint motion pattern.
Materials and Methods
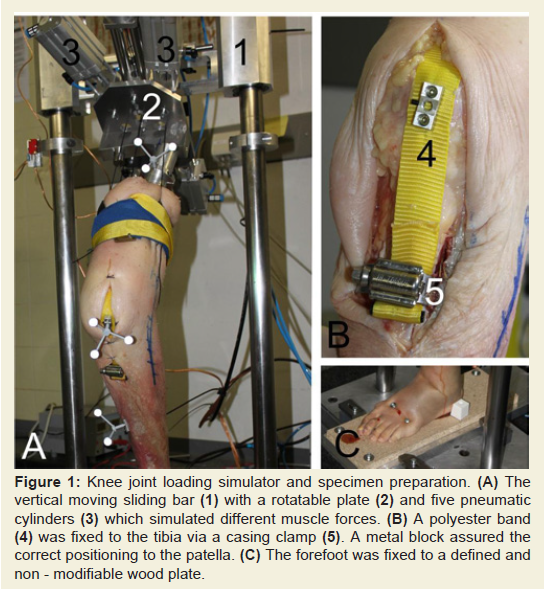
Dynamic squats driven by simulated muscle forces were carried out in a custom - made knee joint loading simulator (
Figure 1A). The kinematics of the intact native tibiofemoral joint (NJ condition) as well as it’s COR were determined as a reference condition. During the experiments a Total Knee Arthroplasty using an implant with a lateral COR (TKA condition) was conducted to successively study the influences on the rotational and translational tibiofemoral joint kinematics. The Ethics Committee of the German Sport University approved the study. The specimens were provided by the Anatomical Institute I, University of Erlangen, Germany and written informed consents of the donors were given for use of this sample in medical research.
Specimen preparation and mounting
Nine fresh frozen cadaver knees (7 left, 2 right; 1 pair, 7 single; 8 female, 1 male) with a mean age at the time of death of 75 years (range 64-91) were used in this investigation. All specimens had intact ligaments without great laxity or evidence of prior surgeries. Several joints showed different grades of osteoarthritis. The alignments of the extended joints were determined in a static upright reference position using a goniometer and characterized as neutral according to the recommendations of Kamath [
23].
The thighs were amputated 300 mm above the knee joint lines, whereas the foot and ankle complexes were kept intact to restore the native individual tibia anatomy and thus the kinematics in the closed kinematic chain. In order to simulate the entire quadriceps muscle, a 15 mm wide polyester band was used. Therefore, an incision from 50 mm above the patella to approximately 30 mm below the tibial tuberosity was done to set a casing clamp near the tibial insertion of the patella ligament as a support for the polyester band (
Figure 1B). This was centrally aligned to the tibial tuberosity, centre-fixed onto the patella and passed through on top of the rectus femoris muscle to the proximal end of the thigh. The skin in front of the knee was closed using sutures. An aluminium tube was fixed to the proximal and of the femur to create a connection to the sliding bar of the knee joint loading simulator, which is described in detail in a later section.
After this preparation, the specimens were mounted into the simulator and the forefoot was fixed to a wood plate using two screws (
Figure 1C). This plate remained fixed at the foot to ensure the same positioning of the specimen in the simulator after the TKA. After capturing the NJ condition the specimens were dismounted for the preparation of the TKA.
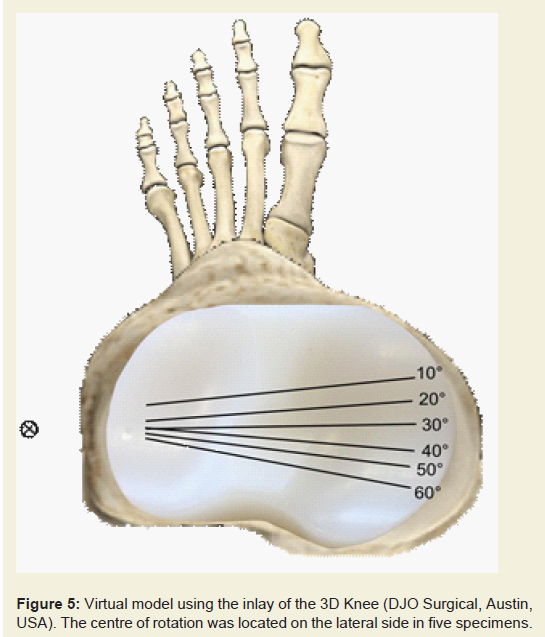
An ACL sacrificing arthroplasty using the 3D Knee system (DJO Surgical, Austin, USA) without the retropatellar component was performed by an experienced senior orthopaedic surgeon according to the manufacturer’s protocol. The knee joint was opened by a medial parapatellar arthrotomy. Intramedullary alignment devices were used to align the femoral components. The posterior aspects of the femoral epicondyles and the epicondylar axis were taken as reference points for proper positioning. Extramedullary instrumentation ensured positioning of the tibial components with a posterior slope approximating the native tibia. The posterior cruciate ligament was retained in all investigated specimens. After implantation the alignment of the components was checked through digital radiographs and a full range of motion tests were performed. The arthrotomy was closed and the specimen was mounted into the knee joint loading simulator, restoring it to the same position as in the earlier experiments.
Knee joint loading simulator
The aluminium tube with the femur was attached to the ball joint and fixed at a rotatable plate on the upper sliding bar of the simulator permitting six degrees-of-freedom positioning. The vertical motion of the sliding bar was guided by a large pneumatic cylinder that produced extension - flexion cycles of the knee joint. Five pneumatic pressure cylinders (ADN, Festo, Esslingen, Germany) applied controlled forces to the muscles and guided the squats via the up and down motion of the sliding bar (Figure 1A). The polyester band was connected to the frontal pneumatic cylinder via a rope and assigned a static force of 500 N to the patella. A belt was strapped around the tissue of the thigh and connected to another four pneumatic cylinders, which applied forces between 80 N and 150 N to the muscles to counteract gravitational forces. The wooden plate with the foot was aligned on the bottom of the simulator so that the ankle joint was positioned below the artificial hip joint of the simulator.
Three custom made metal blocks (
Figure 1B) were fixed to the tibia, the patella and the tube of the femur using small screws. These blocks carried rotational invariant arrays instrumented with three retro - reflective markers used to capture the relative 3D motion of the bones. Six infrared cameras (Nexus 1.5, Vicon Motion System, Oxford, UK) operating at 100 Hz were used. The following pre - determined anatomical reference points were captured for the construction of the femur and tibia coordinate systems: the most prominent points of the medial and lateral femoral epicondyles, the centre point of the ball joint at the proximal femur, and the most medial and lateral point of the tibia plateau as well as the medial and lateral malleolus. Twenty squats with a constant speed and over a predefined range of motion between 10° and 60° of flexion were captured for each experimental condition.
Data processing
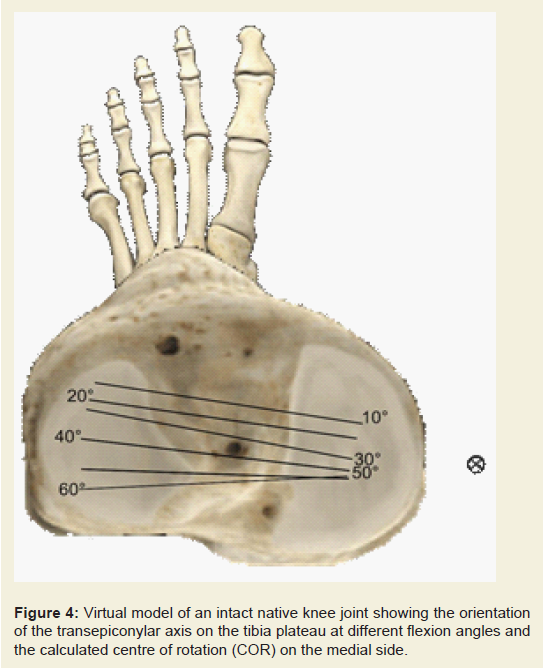
The data processing and calculations of joint motion were done using MATLAB (Version 7.8, The MathWorks Inc., Natick, USA). A recursive fourth order digital Butterworth filter with a cut off frequency of 25 Hz was applied for the marker coordinates. Joint kinematics was calculated using a two segment three-dimensional model of the lower extremity. The transepicondylar axis of the femur was constructed using the most prominent points of the femoral epicondyles. The equations representing this axis in the coordinate system of the tibia were used to calculate the average COR by solving the least - squares system of equations similar to the method described by Banks and Hodge [
24]. Rotational and translational kinematics as well as the COR were calculated for each squat and averaged over the captured cycles.
Results
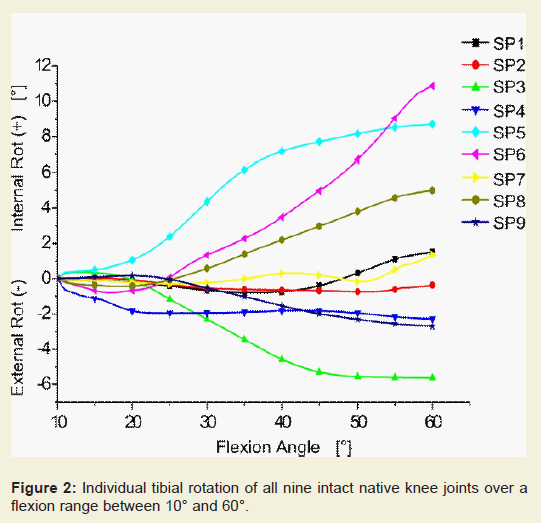
The individual rotational kinematics of all nine investigated specimens revealed a great variance with regards to the direction of rotation and in the amplitude (
Figure 2). Most of the knee joints showed slight tibial rotations relative to the femurs, from 10° to 60° of flexion. Only three joints had greater internal rotations of the tibiae at 60° of flexion, with a gradual increase from the extended joint. Interestingly, the knee joints of one donor (SP3 and SP4) showed external rotations of up to -6° during the flexion cycle.
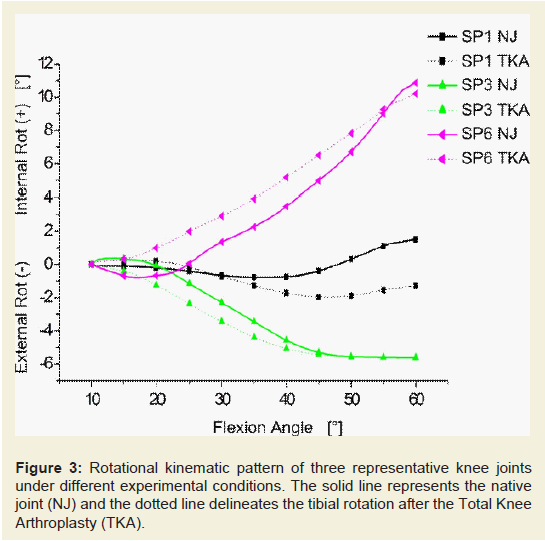
In order to have a better comparison of the tibial rotation between the different experimental conditions, three cases (SP1,SP3,SP6) were chosen as representative examples of all the investigated specimens. In general, total knee replacement did not change the rotational tibiofemoral kinematic pattern in comparison to the native condition (
Figure 3). The differences due to the TKA varied between the investigated specimens, although the overall trend was consistent.
Small differences were found between 10° and 30° of flexion for SP1, whereas greater changes were revealed in the range up to 60° resulting in a difference of 3°. As shown in Figure 3, the impact of the TKA was higher in the flexion range between 10° and 30° for the other two specimens. The difference became smaller with increasing flexion angle, leading to almost the same tibial rotation angle at 60° of flexion.As with the rotational kinematics, a high variance was also found for the translations (
Table 1). During the extension - flexion cycles the anterior - posterior translation of the medial epicondyle was in a range between 3 mm and 9 mm in the NJ condition. The translation of the lateral epicondyle ranged from 4 mm to 20 mm in the same experimental condition.
In comparison to the NJ condition, greater translations of up to 6 mm were found for the medial epicondyle in the TKA condition, except in one specimen. Four of the nine specimens revealed decreased femoral translation between 2 mm and 12 mm on the lateral side compared to the NJ condition. An increased lateral translation of between 3 mm and 8 mm was found in three knee joints, whereas two did not show any translational changes.The calculated COR was found on the medial side of the tibia plateau in eight specimens in the intact native joint condition (Table 1 and Figure 4). Just one knee joint showed a lateral COR. In seven cases the centre was outside of the tibia plateau. A lateral COR was found in five cases for the TKA condition (Table 1 and Figure 5). Interestingly, both knee joints performing an external rotation of the tibia during flexion as well as two joints with a large translation in the NJ condition remained with a medial COR.
Discussion
The chosen approach in the present study represents the first direct measurement of three dimensional tibiofemoral joint kinematics to successively investigate the effects of a TKA with a proposed lateral COR on rotational and translational knee joint kinematics as well as on the COR in comparison to the native condition. The demand for more physiological experimental conditions [
22] in cadaveric studies was met by including the individual anatomy of the ankle joint in a closed kinematic chain experiment. Therefore, presentation of the individual data was chosen instead of averaged motion patterns.
The rotational as well as translational kinematics showed quite a large variance, which is related to individual anatomy, but in a range comparable to other investigations [
25-28]. The external rotation of the tibia during flexion seen in both knee joints of one donor might be unusual but has also been described in other cadaveric studies [
29,30]. It was stated that the reason for this was unclear, but a relation to inter-specimen variability was proposed. Since it was found in both joints of the same donor in the present study, some kind of special kinematic phenotype might be a plausible description. This consideration is related to the fact that, indeed, small alterations in comparison to the native joint were found, but the basic rotation pattern with an external rotation of the tibia also still remained after TKA.
The rotational kinematics after Total Knee Arthroplasty showed almost the same pattern compared to the native joint conditions, only with small offsets. The used implant, with more conformity in the lateral compartment and the ability to allow greater anterior-posterior translation on the medial side reproduced the rotational kinematics, although the COR switched from the medial compartment to the lateral one in five investigated specimens. However, a medial COR was observed in four specimens, which is in contrast to the expected results; but this might be related to the unusual kinematics shown in the NJ condition. On the one hand there might be a relation between the medial COR and the external rotation of the tibia during flexion (SP3 and SP4); on the other hand, to the large translation of the lateral knee joint compartment (SP6 and SP8). External rotation of the tibia seems to be favoured due to the configuration of the medial side of the implant. In addition to this proper axial rotation a large translation even on the lateral compartment seems possible if needed, which is related to the asymmetric femoral component having a constant sagittal radius. This allows a rollback of the femoral condyle in both compartments due to the decreasing articular constraint at higher flexion angles [
31].
A COR on the medial side of the native human knee joint, as it has been found in other cadaveric studies [
26,
32], can be supported by the results of the NJ condition, but an activity dependency found in in vivo studies [
15,
19,20] should be taken into account. The experimental setup of Barnes et al. is not comparable to the approach in this study since they used an open kinematic chain [
32]. We believe that the COR is strongly related to the loading of the knee joint. During squats a medial COR is given due to the greater congruence of the medial compartment resulting from a more adducted knee joint. In contrast to this, the ambulatory load is generally higher leading to more compression and thus to greater friction, keeping the COR in the lateral compartment.
Several limitations of the present study should be mentioned. Using a polyester band to simulate the quadriceps tendon can be seen as a limitation of this study. This approach was chosen in order to have stable force conditions and therefore more comparable experiments. We tried to minimize this error by having the same experienced senior orthopaedic surgeon for the preparation. Furthermore, the amount of simulated muscle force was not as high as in in vivo squats in order to prevent damage to the specimen. Nevertheless, the comparisons of the kinematics are valid and comparable to movements with higher forces, as it has been shown that increased muscle forces do not have an impact on knee joint kinematics [
33]. Further limitations might be present in the fact that the squat started at 10° of flexion; thus, the kinematic information near full extension is missing. This was done in order to prevent hyperextension of the joints, since the force of the hamstrings was too low to counteract the quadriceps force. A realistic simulation of the interaction between agonist and antagonist is not possible in such experiments, since it is not likely to determine their individual force or activation. However, EMG studies showed that the determined hamstring forces during squatting are relatively low, so this might not have a great influence on our results [
34,35].
To conclude our first aim we can state that rotational tibial kinematics might not only be related to the shapes of the articulating surfaces of the knee or the ligamentous and soft tissue constraints but also to the distal part of the tibia. Since the intact ankle joint, as the last part of the kinematic chain in this experiment, can influence the rotation of the tibia, the presented kinematic pattern might be a coupling of the different factors leading to each individual motion pattern. The second aim was achieved by showing that the investigated TKA revealed great accordance in its axial rotation compared to the native joint; even the COR changed its location. The chosen design of the implant allows a rollback of the femoral condyle in both compartments, resulting in the ability to reproduce the motion pattern of the native human knee joint.
The obtained results should be integrated into the future development process of knee implants as well as into the knee joint diagnostics prior to TKA. It is of great importance that the design of the implant is asymmetric, similar to the shape of the native tibiofemoral joint and thus permits the individual movement of the COR. Due to the unconstrained movement and its associated lower friction forces the durability of knee implant might be extended. Furthermore, functional diagnostics prior to TKA should be standardized in order to know the individual kinematics. This might help to achieve a better functional outcome, in the best instance a one - to - one copy of the native kinematics.
Acknowledgements
We thank Prof. Dr. Neuhuber and Dr. Buder from Anatomical Institute I, University of Erlangen, for their support and for providing the specimens. Our great thanks belong to Martin Küsel and Jürgen Geiermann for technical aid. Also many thanks to PD Dr. Jens Dargel from the Clinic for Orthopaedics and Trauma Surgery, University of Cologne for his comments on the manuscript.
References
- Noble PC, Gordon MJ, Weiss JM, Reddix RN, Conditt MA, et al. (2005) Does total knee replacement restore normal knee function? Clin Orthop Relat Res: 157-165.
- Noble PC, Conditt MA, Cook KF, Mathis KB (2006) The john insall award: patient expectations affect satisfaction with total knee arthroplasty. Clin Orthop Relat Res 452: 35-43.
- Kessler S, Käfer W (2007) Comparative assessment of outcome in osteoarthritis of the knee: the utility of knee scores. Acta Chir Orthop Traumatol Cech 74: 332-335.<
- Tanzer M, Smith K, Burnett S (2002) Posterior-stabilized versus cruciate-retaining total knee arthroplasty: balancing the gap. J Arthroplasty 17: 813-819.
- Chalidis BE, Sachinis NP, Papadopoulos P, Petsatodis E, Christodoulou AG, et al. (2011) Long-term results of posterior-cruciate-retaining Genesis I total knee arthroplasty. J Orthop Sci 16: 726-731.
- Parsley BS, Conditt MA, Bertolusso R, Noble PC (2006) Posterior cruciate ligament substitution is not essential for excellent postoperative outcomes in total knee arthroplasty. J Arthroplasty 21 (6 Suppl 2): 127-131.
- Ishida K, Matsumoto T, Tsumura N, Chinzei N, Kitagawa A, et al. (2012) In vivo comparisons of patellofemoral kinematics before and after ADVANCE Medial-Pivot total knee arthroplasty. Int Orthop 36: 2073-2077.
- Hossain F, Patel S, Rhee SJ, Haddad FS (2011) Knee arthroplasty with a medially conforming ball-and-socket tibiofemoral articulation provides better function. Clin Orthop Relat Res 469: 55-63.
- Moonot P, Mu S, Railton GT, Field RE, Banks SA (2009) Tibiofemoral kinematic analysis of knee flexion for a medial pivot knee. Knee Surg Sports Traumatol Arthrosc 17: 927-934.
- Digennaro V, Zambianchi F, Marcovigi A, Mugnai R, Fiacchi F, et al. (2014) Design and kinematics in total knee arthroplasty. Int Orthop 38: 227-233.
- Watanabe T, Ishizuki M, Muneta T, Banks SA (2013) Knee kinematics in anterior cruciate ligament-substituting arthroplasty with or without the posterior cruciate ligament. J Arthroplasty 28: 548-552.
- Elias SG, Freeman MA, Gokcay EI (1990) A correlative study of the geometry and anatomy of the distal femur. Clin Orthop Relat Res 260: 98-103.
- Todo S, Kadoya Y, Moilanen T, Kobayashi A, Yamano Y, et al. (1999) Anteroposterior and rotational movement of femur during knee flexion. Clin Orthop Relat Res 362: 162-170.
- Iwaki H, Pinskerova V, Freeman MA (2000) Tibiofemoral movement 1: the shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J Bone Joint Surg Br 82: 1189-1195.
- Koo S, Andriacchi TP (2008) The knee joint center of rotation is predominantly on the lateral side during normal walking. J Biomech 41: 1269-1273.
- Hoshino Y, Tashman S (2012) Internal tibial rotation during in vivo, dynamic activity induces greater sliding of tibio-femoral joint contact on the medial compartment. Knee Surg Sports Traumatol Arthrosc 20: 1268-1275.
- Kozanek M, Hosseini A, Liu F, Van de Velde SK, Gill TJ, et al. (2009) Tibiofemoral kinematics and condylar motion during the stance phase of gait. J Biomech 42: 1877-1884
- Asano T, Akagi M, Tanaka K, Tamura J, Nakamura T (2001) In vivo three-dimensional knee kinematics using a biplanar image-matching technique. Clin Orthop Relat Res 388: 157-166.
- Yamaguchi S, Gamada K, Sasho T, Kato H, Sonoda M, et al. (2009) In vivo kinematics of anterior cruciate ligament deficient knees during pivot and squat activities. Clin Biomech (Bristol, Avon) 24: 71-76.
- Moro-oka TA, Hamai S, Miura H, Shimoto T, Higaki H, et al. (2008) Dynamic activity dependence of in vivo normal knee kinematics. J Orthop Res 26: 428-434.
- Komistek RD, Dennis DA, Mahfouz M (2003) In vivo fluoroscopic analysis of the normal human knee. Clin Orthop Relat Res: 69-81.
- Varadarajan KM, Harry RE, Johnson T, Li G (2009) Can in vitro systems capture the characteristic differences between the flexion-extension kinematics of the healthy and TKA knee? Med Eng Phys 31: 899-906.
- Kamath AF, Israelite C, Horneff J, Lotke PA (2010) Editorial: What is varus or valgus knee alignment?: a call for a uniform radiographic classification. Clin Orthop Relat Res 468: 1702-1704.
- Banks SA, Hodge WA (2004) 2003 Hap Paul Award paper of the International Society for Technology in Arthroplasty. Design and activity dependence of kinematics in fixed and mobile-bearing knee arthroplasties. J Arthroplasty 19: 809-816.
- D'lima DD, Poole C, Chadha H, Hermida JC, Mahar A, et al. (2001) Quadriceps moment arm and quadriceps forces after total knee arthroplasty. Clin Orthop Relat Res 392: 213-220.
- Yildirim G, Walker PS, Boyer J (2009) Total knees designed for normal kinematics evaluated in an up-and-down crouching machine. J Orthop Res 27: 1022-1027.
- Churchill DL, Incavo SJ, Johnson CC, Beynnon BD (1998) The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res 356: 111-118.
- More RC, Karras BT, Neiman R, Fritschy D, Woo SL, et al. (1993) Hamstrings--an anterior cruciate ligament protagonist: An in vitro study. Am J Sports Med 21: 231-237.
- D'Lima DD, Trice M, Urquhart AG, Colwell CW Jr (2000) Comparison between the kinematics of fixed and rotating bearing knee prostheses. Clin Orthop Relat Res 380: 151-157.
- Patil S, Colwell CW Jr, Ezzet KA, D'Lima DD (2005) Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 87: 332-338.
- Harman MK, Bonin SJ, Leslie CJ, Banks SA, Hodge WA (2014) Total knee arthroplasty designed to accommodate the presence or absence of the posterior cruciate ligament. Adv Orthop 2014: 178156.
- Barnes CL, Blaha JD, DeBoer D, Stemniski P, Obert R, et al. (2012) Assessment of a medial pivot total knee arthroplasty design in a cadaveric knee extension test model. J Arthroplasty 27: 1460-1468.
- Müller O, Lo J, Wünschel M, Obloh C, Wülker N (2009) Simulation of force loaded knee movement in a newly developed in vitro knee simulator. Biomed Tech (Berl) 54: 142-149.
- Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE, et al. (1998) Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc 30: 556-569.
- Isear JA Jr, Erickson JC, Worrell TW (1997) EMG analysis of lower extremity muscle recruitment patterns during an unloaded squat. Med Sci Sports Exerc 29: 532-539.