
Avascular Necrosis of Femoral Head in a 45 year Old Man: A Case Study of an Unnoticed Sickle Cell Disease Patient
Mamuda AA1, Iya AM2 and Bashir Bello2*
- 1Department of Surgery, Bayero University, Nigeria
- 2Department of Surgery, Aminu Kano Teaching Hospital, Nigeria
*Address for Correspondence: Bashir Bello, Department of Surgery, Aminu Kano Teaching Hospital, Kano, Nigeria, Tel: +23409099977557; E-mail: nurubash@yahoo.com
Citation: Mamuda AA, Iya AM, Bello B. Avascular Necrosis of Femoral Head in a 45 year Old Man: A Case Study of an Unnoticed Sickle Cell Disease Patient. The Application of NGS in Prenatal Diagnosis. J Clin Med Case Reports. 2017;4(1): 2.
Copyright © 2017 Mamuda AA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 4, Issue: 1
Submission: 19 December, 2016 | Accepted: 27 January, 2017 | Published: 02 February, 2017
Abstract
Background: Periodic, self-limited episodes of excruciating musculoskeletal pain punctuate the lives of patients with Sickle Cell Disease (SCD) right from childhood. It is very rare for individuals with SCD to be asymptomatic from birth to adulthood.
Objective: The purpose of this study was to present the case of a 45 year old man with an unnoticed sickle disease following Avascular Necrosis (AVN) of the femoral head.
Case study: The patient is a 45 year old civil servant, who presented with complaints of pains of the right hip of six (6) months duration. He was involved in a Road Traffic Accident (RTA) one month prior to onset of pain, however no associated fractures was seen at that time. No history of prolonged exposure to steroids or radiation. He is not a known sickle cell disease patient and does not smoke cigarette nor ingest alcohol.
Methodology and results: Physical examination revealed a well preserved man with no sickle cell disease habitus. Laboratory findings of FBC and ESR were normal. Plain radiographs of the pelvis and hips showed hypoplasia, sclerosis, articular marginal irregularity and subarticular cystic changes, all consistent with stage III (Ficat and Arlet). This prompted further evaluation of the patient to identify the cause of the AVN. The patient was then sent for genotyping; and a hemoglobin electrophoresis: (Hb SS+F) was noted.
Conclusion: SCD can be diagnosed at adulthood for the first time due to asymptomatic presentation. Patient was therefore educated on the nature and progression of the disease and counseled for hemiarthroplasty of right hip. He was then placed on NSAIDS, reduced weight bearing on the hips and gradual range of motion exercises.
Keywords
Sickle cell disease; Avascular necrosis; Hip joint
Introduction
Sickle Cell Disease (SCD) is a multisystem disease associated with episodes of acute illness and progressive organ damage, and one of the most common monogenic disorders worldwide, affecting an estimated 30 million people. SCD represents a major public health problem because of its associated morbidity and mortality [1,2].
In low-resource countries, like Nigeria, more than 50% of children younger than 5 years of age die due to complications of SCD [3].
Avascular necrosis is characterized by osseous cell death due to vascular compromise [4]. Avascular necrosis of bone results generally from corticosteroid use, trauma, pancreatitis, alcoholism, gout, radiation, sickle cell disease, infiltrative diseases (e.g. Gaucher’s disease), and Caisson disease [4,5].
Akinyola et al. affirmed that the earliest symptom of AVN is pain at joint at first when bearing weight on affected joint, then later even at rest [3,6]. Later in the disease, joint stiffness, osteoarthritis and deformity may occur.
MRI is the most reliable way of detecting early changes while late features are evident on plain radiographs [7].
Treatment is challenging and better results are achieved when a multidisciplinary approach is taken. Literatures on Avascular Necrosis of the Femoral Head (AVN FH) presenting as the first pointer to sickle cell disease are still dearth. Findings of this present study will help physicians see possibilities of evaluating adult with unexplained hip pain to rule out SCD.
Case Report
The patient is a 45 year old civil servant, who presented with complaints of pains of the right hip of six (6) months duration. He described the pain as dull aching worsened with walking long distances and on prolonged standing, relived by simple analgesics. He was involved in a Road Traffic Accident (RTA) one month prior to onset of pain, however no associated fractures. No history of prolonged exposure to steroids or radiation. He is not a known sickle cell disease patient. He does not smoke cigarette or ingest alcoholic beverages.
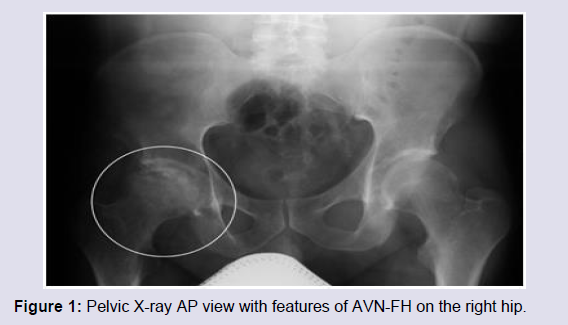
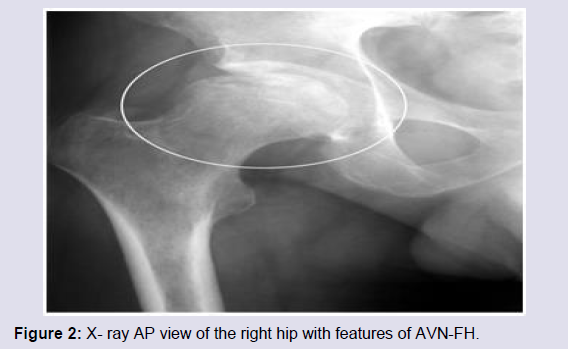
General physical examination revealed a well preserved man with no sickle cell disease habitus, lower limb examination was unremarkably normal. Full blood count results (Haemoglobin: 13.9 g/dl, White Blood Cell: 4.1*109/l, Platelet: 142*109/l), ESR: 10 mm/h, Haemoglobin electrophoresis: Hb SS+F) were noted. Plain radiographs of the pelvis and hips showed hypoplasia, sclerosis, articular marginal irregularity and subarticular cystic changes, all consistent with stage III (Ficat and Arlet).
Patient was educated on the nature and progression of the disease and counseled for right hemiarthroplasty of right hip. He was then placed on NSAIDS, reduced weight bearing on the hips and range of movement exercises.
Discussion
Tailor et al. explained that the clinical course of sickle cell disease is punctuated by acute painful episodes traditionally referred to as ‘crises’ which are the hallmark of the disease [6]. They further stated that the clinical consequences of sickle cell crises are diverse and have been the subject of numerous varied reports in the medical literature. According to Frenette and Atweh SCD first manifests in children or adolescents [7]. Patients mostly present with hemolyticanemia, jaundice, repeated vaso occlusive crisis, hand foot syndrome, acute chest syndromes, and splenic sequestration crisis etc. They can also get repeated infections like pneumonias, osteomyelitis, dactylitis etc. however, this patient had no presentation of any of the above conditions except for the radiographic features of AVN-FH.
Avascular necrosis of the femoral head has been described as a frequent out come in patients with sickle cell disease with a prevalence of up to 15.9% and a mean age a presentation at 38 years [3]. This patient however presented in an unusual way. First, he presented for the first time with sickle cell related illness at the age of 45 years, with no significant past medical history. There was no history of any possible use of corticosteroids or trauma due to a fall or road traffic accident. It was only on the subsequent follow-up laboratory work up, he was co-incidentally noted to have Hb SS and Hb F which was the only pointer to the cause of the AVN-FH. Thus, the atypical presentation of sickle cell disease in this patient at 45 years may be attributed to the persistence of Hb F.
Radiological features of osteonecrosis generally involve collapse of the articular cortex, fragmentation, mottled trabecular pattern, sclerosis, subchondral cysts, and/or subchondral fracture [4]. This patient’s radiographs demonstrated the presence of osteonecrosis of the right hip (Figure 1 and 2).
Patient was therefore educated on the nature and progression of the disease and counseled for hemiarthroplasty of right hip. He was then placed on NSAIDS, reduced weight bearing on the hips and gradual range of motion exercises.
The patient is still being followed up with the above mentioned conservative treatment line until when the pain will become unbearable and the patient psychologically stable for the surgical procedure.
Fye et al. stated that the treatment of AVN-FH is mainly surgical and generally involves a total hip replacement or arthroplasty for end-stage femoral head osteonecrosis using either a cemented or cementless prosthesis [8]. Researchers have reported improved outcomes with cementless total hip arthroplasties for patients with femoral head osteonecrosis. This patient is eventually being planned for it whenever the surgery is due [8-10].
Conclusion
SCD can be diagnosed at adulthood for the first time due to asymptomatic presentation.
References
- Inati A, Koussa S, Taher A, Perrine S (2008) Sickle cell disease: new insights into pathophysiology and treatment. Pediatr Ann 37: 311-321.
- Rees DC, Williams TH, Gladwin MT (2010) Sickle-cell disease. Lancet 376: 2018-2031.
- Akinyola AL, Adediran IA, Asaleye CM (2007) Avascular necrosis of femoral head in sickle cell disease in Nigeria: a retrospective study. Niger Postgrad Med J 14: 217-220.
- Yochum TR, Rowe LJ (1996) Essentials of skeletal radiology, (2ndedn). Williams & Wilkins, Baltimore, pp. 1260-1263.
- Tierney LM, Papadakis MA, McPhee SJ (1998) Current Medical diagnosis and treatment, (36thedn). Appleton & Lange, Stamford, pp. 798-799.
- Tailor HJ, Hathila RN, Patel PR (2015) Death due to sickle cell anaemia, an autopsy diagnosis: a study at a tertiary care hospital. Int J Res Med Sci 3: 944-947.
- Frenette PS, Atweh GF (2007) Sickle cell disease: old discoveries, new concepts, and future promise. J Clin Invest 117: 850-858.
- Fye MA, Huo MH, Zatorski LE, Keggi KJ (1998) Total hip arthroplasty performed without cement in patients with femoral head osteonecrosis who are less than 50 years old. J Arthroplasty 13: 876-881.
- Piston RW, Engh CA, De Carvalho PI, Suthers K (1994) Osteonecrosis of the femoral head treated with total hip arthroplasty without cement. J Bone Joint Surg Am 76: 202-214.
- Phillips FM, Pottenger LA, Finn HA, Vandermolen J (1994) Cementless total hip arthroplasty in patients with steroid-induced avascular necrosis of the hip. A 62-month follow-up study. Clin Orhop Relat Res: 147-154.