
Co-Infection of Cryptococcal and Multidrug Resistant Tuberculous Meningitis in Immunocompetent Patient
Urvashi B. Singh1*, Gautam Hitender1, Venugopal Shwetha1, Porwal Chhavi1, Rana Tanu1, Xess Immaculata1, Bhatia Rohit2 and Vasantha Padma2
- 1Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India
- 2Department of Neurology, All India Institute of Medical Sciences, New Delhi, India
*Address for Correspondence: Urvashi B. Singh, Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India, Tel: +91-11-26546436; Fax: +91-11-26588663; E-mail: drurvashi@gmail.com
Citation: Singh UB, Hitender G, Shwetha V, Chhavi P, Tanu R, et al. Co-Infection of Cryptococcal and Multidrug Resistant Tuberculous Meningitis in Immunocompetent Patient. The Application of NGS in Prenatal Diagnosis. J Clin Med Case Reports. 2017;4(1): 3.
Copyright © 2017 Singh UB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 4, Issue: 1
Submission: 21 November, 2016 | Accepted: 05 January, 2017 | Published: 13 January, 2017
Abstract
A rare, previously unreported case of concurrent central nervous system infection with Cryptococcus neoformans and multi-drug resistant Mycobacterium tuberculosis in a 27-year-old immunocompetent female patient who reported to a tertiary care centre in North India. Various diagnostic and case management difficulties encountered for the management of this case have been highlighted. Correct and complete etiological identification, enabling early, appropriate treatment in patients with concomitant infections may pose a diagnostic dilemma. The case highlights the need to maintain an increased level of clinical suspicion for co-infections with tuberculosis (TB), (especially in TB meningitis), even if there are no obvious signs of immunodeficiency, thereby indicating that TB could be the cause for immunosuppression, hence paving way for opportunistic infections.
Keywords
MDR tuberculous meningitis; Cryptococcal meningitis; Immunocompetent
Case History
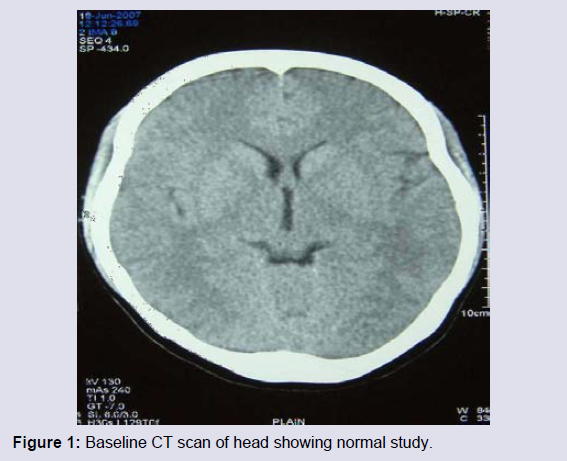
A 27-year-old female, resident of North Eastern part of India had history of fever, headache and vomiting for 2-3 days in June, 2007. She was treated with intravenous antibiotics for 7 days and her symptoms subsided. She remained asymptomatic for the next three months, but developed fever, headache, vomiting again. Her cerebrospinal fluid (CSF) adenosine deaminase (ADA) level was increased, though computer tomography (CT) scan of the head was normal (Figure 1). At this time, CSF Ziehl Neelsen staining was negative for acid-fast bacilli and India ink staining was negative for any capsulated structure. First line anti-tubercular treatment (ATT) (isoniazid, rifampicin, pyrazinamide and ethambutol) was started on the basis of clinical presentation and elevated ADA levels. ADA is a rapid, inexpensive and sensitive test in the diagnosis of TBM. However, despite the sensitivity and specificity of CSF ADA, it should be corroborated with AFB smear and CSF PCR [1]. Over the next few weeks she improved clinically and continued regular intake of the drugs.
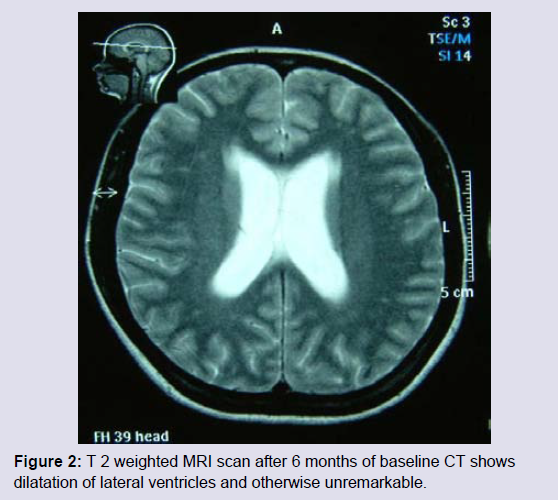
However, 2 months after initiating ATT, she had mild derangements in liver function tests. Hence, rifampicin and pyrazinamide were stopped, for few days. Though symptoms subsided initially, she continued to have loss of appetite. She consulted another physician after 6 months on ATT and was advised magnetic resonance imaging (MRI) scan of the head that showed symmetrical hydrocephalus (Figure 2). Ofloxacin was added to her treatment regimen but even on this regimen for 2 months, her condition worsened with severe headache and intractable vomiting.
With this background the patient reported to the department of Neurology, in April 2008. Her general and nervous system examinations were normal except for bilateral papilloedema. The routine investigations were unremarkable except for rise in erythrocyte sedimentation ratio (ESR). The CSF analysis this time showed predominant lymphocytosis (60% lymphocytes in WBC differential), increased proteins (145 mg/dL) and decreased sugars (10 mg/dL). The Gram staining, routine cultures for bacteria, acid fast staining and polymerase chain reaction (PCR) for M. tuberculosis, India ink staining for Cryptococcus neoformans were all negative. The CSF was positive for Cryptococcal antigen by latex agglutination. The liquid culture of CSF grew M. tuberculosis in 2 weeks. Meanwhile the culture for C. neoformans was also positive. The patient was negative for HIV testing and tests for her immunological profile were within normal limits. There was no lymphopenia. Her absolute CD4 T-lymphocyte count was 900/mm3, CD8 count was 400/mm3 and CD4 to CD8 ratio was > 2 which published literature signified that the patient had a healthy immune system [2]. The patient was not on steroids till she reported to our institute, had no haematological or other malignancy, no history of transplantation, not on any immunosuppressive drug, not a diabetic, no history of smoking or alcohol consumption. There was no evidence for tuberculosis elsewhere in the body.
During the course of hospital stay, she was treated with intravenous amphotericin B (one month), dexamethasone and first line antitubercular drugs under treatment failure category of previously treated cases and streptomycin was added under that. The patient tolerated the treatment well and her clinical condition improved. The patient was discharged after one month with the advice to continue the anti-tubercular and oral antifungal drugs (fluconazole).
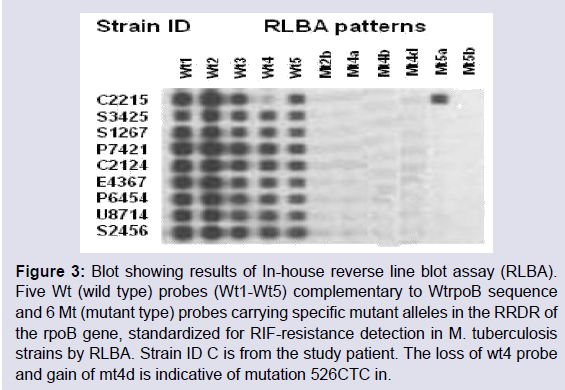
She was reviewed after 1 month, had no complaints and was having good compliance to drugs. Her examination and investigations were within normal limits. Anti-tuberculous drug susceptibility done on the culture isolate from the CSF, using an in-house reverse line blot assay (RLBA) showed resistance to rifampicin, which is considered as a surrogate marker for multi-drug resistance in Mycobacterium tuberculosis (Figure 3) [3,4]. However, since she was clinically improving, no change was made to the treatment. She had regular follow up and remained asymptomatic and oral antifungal (fluconazole) was stopped after 10 weeks of initiation and continued on ATT. At 6 months follow up also she remained asymptomatic, her examination was within normal limits and advised for continuing ATT. After about a year of enrolment at our institute, she was lost to follow up.
Discussion
Chronic meningitis in adults is frequently encountered in clinical practice. The etiologies include both infectious and non-infectious causes. However, there are few reports describing tuberculous and cryptococcal meningitis co-infections in apparently immunecompetent persons. We describe cryptococcal meningitis concurrent to tuberculous meningitis in an immunocompetent individual.
Silber, et al. described the dual infection with cryptococcal meningitis and tuberculous meningitis in HIV-1 seropositive patients [5]. The simultaneous occurrences of cryptococcal infection with tuberculosis involving various organs have been reported in the literature [6]. Till date cases of the coexistence of both tuberculous meningitis and cryptococcal meningitis in apparently immunocompetent persons have been reported by various authors [7-9]. To the best of our knowledge this is the first case report where cryptococcal meningitis occurred concurrently in an apparently immunocompetent, HIV seronegative patient with tuberculous meningitis. Incidentally, the patient reported also showed resistance to first line ATT drug (rifampicin). Northeast states of India have specific issues related to TB, which make the control program implementation challenging in these areas, due to poor accessibility, difficult geographical terrain, weak infrastructure and socio-political issues. One study among MDR-TB suspects in northeast region of India have found MDR-TB in the range of 30% [10] which highlights that there is increased incidence of drug resistant TB in north east regions and improved surveillance activities are required in this part of India.
Cryptococcosis in man is a widely disseminated disease and the organism has been isolated from samples as diverse as urine and joint fluid. A lowered host resistance due to a pre-existing chronic disease may be a triggering factor. Some authors have shown that cryptococcal meningitis is more likely to occur in patients with underlying immunosuppressive conditions [5,11]. The cryptococcal meningitis in HIV patients usually manifests when they have lower CD4 cell count which contributes to subtle symptoms and CSF findings in them [12].
Cryptococcal meningitis though occurs in immunocompromised patients, it has also been reported in apparently immunocompetent persons [13]. Stockstill MT, et al. observed that in his study, all the patients with cryptococcal meningitis had an underlying immunosuppressive condition such as corticosteroid therapy, cytotoxic drug therapy, hematologic malignancy, renal transplant, alcohol abuse, diabetes mellitus and sarcoidosis [11].
The cause for dual infection due to C. neoformans and M. tuberculosis remains elusive. Some have hypothesized that the cell mediated immunity is altered in tuberculous infection and this might predispose to fungal infection [8]. Others opined that the C. neoformans causes invasive infection when host-parasite relationship is altered due to the underlying causes in the host [10]. In the literature three cases of co-infection of tuberculous and cryptococcal meningitis have been reported in immunocompetent persons [7-9]. In the above case of concurrent central nervous system infection with Cryptococcus neoformans and multi-drug resistant Mycobacterium tuberculosis, all the immunologic studies were normal; a chronic tuberculosis infection may have favored the development of the cryptococcal meningitis.
The case highlights that an increased level of clinical suspicion should be kept to rule out co-infections with tuberculosis, even if there are no obvious signs of immunodeficiency. Emphasis should be given to correct and complete etiological identification, allowing appropriate and timely treatment.
References
- Chacko F, Modi M, Lal V, Prabhakar S, Rana SV, et al. (2010) Diagnostic efficacy of adenosine deaminase levels in cerebrospinal fluid in patients of tubercular meningitis: a comparison with PCR for Mycobacterium tuberculosis. Ann Neurosci 17: 126-130.
- Das BR, Bhanushali AA, Khadapkar R, Jeswani KD, Bhavsar M, et al. (2008) Reference ranges for lymphocyte subsets in adults from western India: influence of sex, age and method of enumeration. Indian J Med Sci 62: 397-406.
- Suresh N, Singh UB, Arora J, Pande JN, Seth P, et al. (2006) Rapid detection of rifampicin-resistant Mycobacterium tuberculosis by in-house, reverse line blot assay. Diagn Microbiol Infect Dis 56: 133-140.
- Traore H, Fissette K, Bastian I, Devleeschouwer M, Portaels F (2000) Detection of rifampicin resistance in Mycobacterium tuberculosis isolates from diverse countries by a commercial line probe assay as an initial indicator of multidrug resistance. Int J Tuberc Lung Dis 4: 481-484.
- Silber E, Sonnenberg P, Koornhof HJ, Morris L, Saffer D (1998) Dual infective pathology in patients with cryptococcal meningitis. Neurology 51: 1213 -1215.
- Kiertiburanakul S, Sungkanuparph S, Malathum K, Pracharktam R (2003) Concomitant Tuberculous and Cryptococcal thyroid abscess in a human immunodeficiency virus-infected patient. Scand J Infect Dis 35: 68-70.
- Nanda SP, Kass I, Cohn M, Dressler SH (1957) Coexistence of tuberculous and cryptococcal meningitis. Pediatrics 209(1 Part 1): 45-52.
- Gómez-Aranda F, López-Domínguez JM, Muñoz Málaga A, Blanco Ollero A (1993) Meningitis simultaneously due to Cryptococcus neoformans and Mycobacterium tuberculosis. Clin Infect Dis 16: 588-589.
- Manfredi R, Calza L (2008) Severe brain co-infection with Cryptococcus neoformans and Mycobacterium tuberculosis in a young, otherwise healthy student recently immigrated from China. Int J Infect Dis 12: 438-441.
- Singhal R, Myneedu VP, Arora J, Singh N, Sah GC, et al. (2014) Detection of multi-drug resistance & characterization of mutations in Mycobacterium tuberculosis isolates from North-Eastern states of India using GenoType MTBDRplus assay. Indian J Med Res 140: 501-506.
- Stockstill MT, Kauffman CA (1983) Comparison of cryptococcal and tuberculous meningitis. Arch Neurol 40: 81-85.
- 12.Sanchez-Portocarrero J, Perez-Cecilia E, Jimenez-Escrig A, Martin-Rabadán P, Roca V, et al. (1996) Tuberculous meningitis. Clinical characteristics and comparison with cryptococcal meningitis in patients with human immunodeficiency virus infection. Arch Neurol 53: 671-676.
- Lui G, Lee N, Ip M, Choi KW, Tso YK, et al. (2006) Cryptococcosis in apparently immunocompetent patients. QJM 99: 143-151.