
Journal of Clinical & Medical Case Reports
Download PDF
Case Report
*Address for Correspondence: Vincent Yaba Shidali, Department of Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, Tel: +2348065601165; E-mail: vincentshidali@gmail.com
Citation: Shidali VY, Oyati AI, Isa MS, Obiako RO. Tricuspid Valve Endocarditis due to Klebsiella Specie in a Non-Intravenous Drug User - A Case Report and Review of Current Literature. J Clin Med Case Reports. 2016;3(2): 3.
Copyright © 2016 Shidali VY, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 2
Submission: 16 August, 2016 | Accepted: 13 October, 2016 | Published: 20 October, 2016

 A diagnosis of congestive cardiac failure secondary to rheumatic valvular heart disease complicated by tricuspid valve sub-acute bacterial endocarditis was made using the modified Duke’s criteria (1 major criterion and 5 minor criteria). She was placed on parenteral levofloxacin (she initially had ceftriaxone before blood culture result) and gentamycin with anti- heart failure drugs. The fever subsided and the patient sustained general recovery. However, at 3 months of follow up, patient is still in NYHA III cardiac failure and has developed right-sided pleural effusion (Figure 3).
A diagnosis of congestive cardiac failure secondary to rheumatic valvular heart disease complicated by tricuspid valve sub-acute bacterial endocarditis was made using the modified Duke’s criteria (1 major criterion and 5 minor criteria). She was placed on parenteral levofloxacin (she initially had ceftriaxone before blood culture result) and gentamycin with anti- heart failure drugs. The fever subsided and the patient sustained general recovery. However, at 3 months of follow up, patient is still in NYHA III cardiac failure and has developed right-sided pleural effusion (Figure 3).

Tricuspid Valve Endocarditis due to Klebsiella Specie in a Non-Intravenous Drug User - A Case Report and Review of Current Literature
Vincent Yaba Shidali*, Albert Imhoagene Oyati, Muhammad Sani Isa and Reginald Onyeadumarakwe Obiako
- Department of Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria
*Address for Correspondence: Vincent Yaba Shidali, Department of Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, Tel: +2348065601165; E-mail: vincentshidali@gmail.com
Citation: Shidali VY, Oyati AI, Isa MS, Obiako RO. Tricuspid Valve Endocarditis due to Klebsiella Specie in a Non-Intravenous Drug User - A Case Report and Review of Current Literature. J Clin Med Case Reports. 2016;3(2): 3.
Copyright © 2016 Shidali VY, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical & Medical Case Reports | ISSN: 2332-4120 | Volume: 3, Issue: 2
Submission: 16 August, 2016 | Accepted: 13 October, 2016 | Published: 20 October, 2016
Abstract
Tricuspid valve (TV) endocarditis is known to be predominant among intravenous drug users (IDU) commonly due to staphylococcus species. Isolation of Klebsiella species from a TV endocarditis is an uncommon finding. Endocarditis leading to heart failureportends a worse prognosis and is an indication for surgical intervention.In this report, a 20 year old female non-intravenous drug user (NIDU) in peuperium presented with heart failure precipitated by sepsis. Further evaluation revealed background rheumatic valvular heart disease with tricuspid valve endocarditis caused by Klebsiella species. She responded to antibiotics. However, after 3 months of discharge, she presented with significant morbidity from persistent heart failure and pleural effusion.
Keywords
Non-Intravenous drug user; Tricuspid valve endocarditis; Klebsiella species; Heart failureIntroduction
Infective endocarditis is an infection of the cardiac endothelium, macroscopically seen as vegetation [1]. In the general population (including NIDU) and inthe presence of rheumatic valve disease, endocarditis occurs more frequently on the mitral valve followed by aortic valve [2,3]. The incidence has remained constant over the last 30 years but the spectrum of underlying cardiac conditions and the causative organisms have changed over time [1,2].In Intravenous Drug Users (IDUs), endocarditis is mainly on the tricuspid valve. Tricuspid valve endocarditis has also been reported among the general population, including 9% of NIDUs [4,5]. Staphylococcus aureus has been implicated in most tricuspid valve endocarditis, while Escherichia coli and Pseudomonas aeuroginosa have been reported in only sporadic cases [6]. However, Klebsiella species is an uncommon cause of endocarditis. This may be due to its poor adherence to cardiac valves compared to other organisms commonly responsible for the disease [7].
In this report, we present a case of isolated tricuspid valve endocarditis in a NIDU caused by Klebsiella species.
Case Report
A 20 year old primiparous female referred on account of 7 weeks history of continuous fever and productive cough with 5 weeks of progressive breathlessness and leg swelling. Breathlessness was associated with paroxysmal nocturnal dyspnea, orthopnea and subsequent dyspnea at rest; swelling was limited to the legs. Systemic review was not remarkable except for 3 weeks history of jaundice. Symptoms started 1 week after delivery. There was no prior history of cardiac disease or recent surgical procedure. She had intravenous medications and 3 units of whole blood before referral.On examination, she was acutely ill-looking, cachectic, pale, icteric and febrile (38.4 °C). She had bilateral pitting leg oedema but no peripheral stigmata of infective endocarditis. Her pulse rate was 140 beats/min, regular, small volume; blood pressure of 130/110 mmHg, distended neck veins, soft S1, S2, S3 gallop rhythm and murmur of tricuspid regurgitation. She also had tachypnea with chest crepitations, tender soft hepatomegaly and ascites.
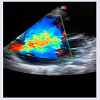
Laboratory investigations revealed PCV of 23%, WBC of 20.7 x 109/L with neutrophilia (89%) and reduced platelet count 139x109/L. Urea was 9 mmol/L, Na+ 134 mmol/L, HCO3 -16 mmol/L while other findings were within normal range. One of two blood culture samples yielded Klebsiella species sensitive to levofloxacin, ofloxacin, ceftriaxone and gentamycin. INR, urinalysis, urine/sputum MCS results were not remarkable. Chest X-ray (CXR) revealed bilateral lung infiltrates while ECG showed sinus tachycardia. Trans thoracic echocardiography (Figures 1 and 2) showed markedly thickened mitral and tricuspid valves, dilated right cardiac chambers with severe TR, mild MR and AR. There was multiple oscillating vegetation on the TV of which the largest measured 0.9 x 0.6 cm.
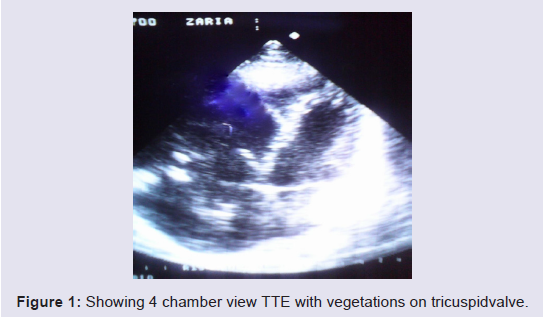
Figure 1:Showing 4 chamber view TTE with vegetations on tricuspidvalve.
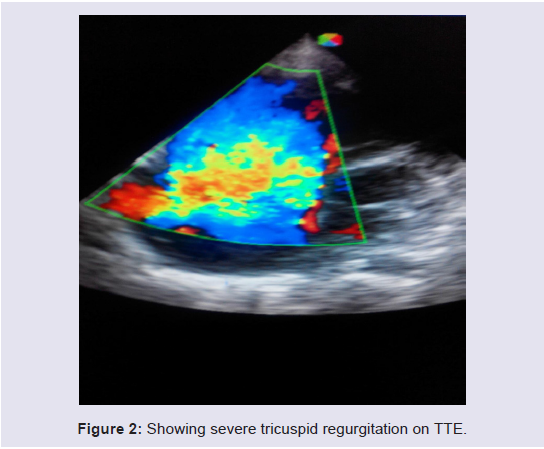
Figure 2: Showing severe tricuspid regurgitation on TTE.
Figure 3: Showing CXR with cardiomegaly and pleural effusion.
Discussion
A search for endocarditis is usually the result of a high index of suspicion especially in patients without established known risks such as prosthetic valve, congenital heart disease, IDU, recent cardiac surgery or rheumatic valvular heart disease [3]. With the persistent prevalence of rheumatic heart disease in developing countries [2], this suspicion must be strengthened although in the index case, a prior knowledge of a RHD was lacking. It is also noteworthy to mention that combined mitral and tricuspid valve involvement is uncommon. In a report of 47 cases of rheumatic heart disease by Danbauchi et al. no organic tricuspid valve lesion could be proven from the same centre [8].Thomas MG et al., reported 6 cases (collated from reports in the English literature over 44 yrs) of Klebsiella endocarditis but only one involved the tricuspid valve following bacteremia from a transvenous catheter [9]. Ana Ravilla et al. in an attempt to investigate the current frequency of right-sided endocarditis in NIDU reported 17 cases among which only one patient had tricuspid valve Klebsiella endocarditis [10].
The suspected source of sepsis was the chest or genitourinary tract. It was however apparent that sepsis was not adequately treated before referral thereby predisposing the susceptible valve. In fact, high levels of bacteremia have been associated with right-sided endocarditis [11]. In a study of non-drug addict patients with right-sided endocarditis, inadequately treated sepsis (post abortion, placental abruption and genitourinary) was found to be the most common cause of right sided vegetation [12,13]. It is however not clear why an endocarditis associated with sepsis in a patient with both mitral and tricuspid valve disease was restricted to the latter. This isolated nature of the disease is further strengthened by the absence of systemic immunological and vascular phenomena.
The persistent showers of emboli to the pulmonary bed noted as lung infiltrates on CXR may have contributed to the dilated right cardiac chambers alongside the effect of RV overload from incompetent TV (Figures 1 and 2). Large vegetation, valve perforation and root abscess as noted by Thomas MG et al. in his review of 6 Klebsiella endocarditis were not a feature in this patient. A recent report by Ji-Ae Hwang et al. of a community-acquired Klebsiella pneumoniae caused a pneumonia, liver abscess and endocarditis which involved the mitral and tricuspid valve [14]. Our case resulted in a pneumonia and endocarditis only.
Identification of organism from culture with sensitivity pattern is an important tool in the management of endocarditis. Other laboratory results were consistent with a septic patient in heart failure. The patient responded to levofloxacin given for at least 6 weeks and gentamycin at the initial period of treatment. Despite effective antibiotic treatment, specific complications that may worsen outcome must be addressed. It is well established that outcome is better in right-sided endocarditis but the presence of heart failure is an indication for surgical intervention even in the presence of co-morbidity [1]. This management modality has largely remained elusive for patients in most developing nations thereby leading to a bad outcome such as persistent heart failure and pleural effusion (Figure 3) as was seen three months after treatment in the index case.
In conclusion, the case demonstrates the possibility of unusual organisms affecting tricuspid valve in non- intravenous drug users who traditionally are not prone to tricuspid valve disease. Also, comprehensive management including valve repairs/replacement is critical to achieving favorable outcomes with minimal morbidity.
References
- Griffin BP (2013) Manual of cardiovascular medicine. 4th edn, Lippincott William & Wilkins, Philadelphia, USA.
- Murphy JG, Lloyd MA, Clinic M (2007) Mayor clinic cardiology: concise textbook. 3rd edn, Minnesota, USA.
- Bonow RO, Mann DL, Zipes DP, Libby P (2012) Braunwald’s heart disease: a textbook of cardiovascular medicine. 9th edn, Saunders Elservier, Philadelphia, USA.
- Chambers HF, Morris DL, Tauber MG, Modin G (1987) Cocaine use and the risk for endocarditis in intravenous drug users. Ann Intern Med 106: 833-836.
- Chambers HF, Korzeniowski OM, Sande MA (1983) Staphylococcus aureus endocarditis: clinical manifestations in addicts and nonaddicts. Medicine (Baltimore) 62: 170-177.
- Morpeth S, Murdoch D, Cabell CH, Karchmer AW, Pappas P, et al. (2007) Non-HACEK gram-negative bacillus endocarditis. Ann Intern Med 147: 829-835.
- Gould K, Ramirez-Ronda CH, Holmes RK, Sandford JP (1975) Adherence of bacteria to heart valve in vitro. J Clin Invest 56: 1364-1370.
- Danbauchi SS, Alhassan MA, David SO, Wammanda R, Oyati IA (2004) Spectrum of rheumatic heart disease in Zaria, Northern Nigeria. Ann Afr Med 3: 17-21.
- Thomas MG, Rowland-Jones S, Smyth E (1989) Klebsiella pneumonia endocarditis. J R Soc Med 82: 114-115.
- Revilla A, Lopez J, Villacorta E, Gomez I, Sevilla T, et al. (2008) Isolated right-sided valvular endocarditis in non-intravenous drug users. Rev Esp Cardiol 61: 1253-1259.
- Frontera JA, Gradon JD (2000) Right-side endocarditis in injection drug users: review of proposed mechanisms of pathogenesis. Clin Infect Dis 30: 374-379.
- Naidoo DP (1993) Right-sided endocarditis in the non-drug addict. Postgrad Med J 69: 615-620.
- Grover A, Anand IS, Varma J, Choudhury R, Khattri HN, et al. (1991) Profile of right-sided endocarditis: an Indian experience. Int J Cardiol 33: 83-88.
- Hwang JA, Her C, Kim YW (2013) Endocarditis caused by community-acquired Klebsiella pneumoniae Infection. Korean J Crit Care Med 28: 41-45.