
Research Article
Diagnostic Performance of the Rutgers Alcohol Problem Index (RAPI) in Detecting DSM-5 Alcohol Use Disorders among College Students
Brett T. Hagman*
- Division of Treatment and Recovery Research, National Institute on Alcohol Abuse and Alcoholism, USA
*Address for Correspondence: Brett T. Hagman, Division of Treatment and Recovery Research, National Institute on Alcohol Abuse and Alcoholism, 5635 Fishers Lane, Room 2044, Bethesda, MD 20892, USA, Tel: 301-443-0638; E-mail: brett.hagman@nih.gov
Citation: Hagman BT. Diagnostic Performance of the Rutgers Alcohol Problem Index (RAPI) in Detecting DSM-5 Alcohol Use Disorders among College Students. J Addiction Prevention. 2017;5(2): 7.
Copyright: © 2017 Hagman BT. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Addiction & Prevention | ISSN: 2330-0396 | Volume: 5, Issue: 2
Submission: 26 May, 2017 | Accepted: 04 July, 2017 | Published: 13 July, 2017
Keywords
College student; DSM-5 AUD; Alcohol problems; Alcohol use; Diagnosis
Abstract
Background and objectives: The DSM-5 Alcohol Use Disorder criteria (AUD) have been modified to reflect a single diagnosis, which may alter how AUDs are detected within our screening measures. The Rutgers Alcohol Problem Index (RAPI) is one of the most widely used screening measures of alcohol problems in college students. The present study sought to evaluate the diagnostic performance of the RAPI in detecting DSM-5 AUDs in college students.
Methods: Participants (n = 396; 52% male) were past year drinkers in college either full or part-time. They were asked to fill out a one-hour anonymous packet of questionnaires.
Results: The RAPI performed slightly better in the detection of DSM-5 AUDs (AUROC = 0.828; SE = 0.20) in comparison to any DSM-IV AUD (0.791; SE = 0.022; 95% CI, 0.748 - 0.835). The performance of the RAPI was lower when detecting frequency (AUROC = 0.719; SE = 0.025) or quantity of alcohol use (AUROC = 0.758; SE = 0.024) in comparison to detecting DSM-5 AUDs. Gender differences emerged in the identification of optimal RAPI cut-off scores. Findings indicate that an overall RAPI score of 4 be used for female college students and an overall score of 6 be used for male college students in the detection of DSM-5 AUDs.
Discussion and conclusions: This is the first study to evaluate the performance of the RAPI in identifying DSM-5 AUDs in college students. Study findings indicate that the RAPI provides reasonably good discrimination in classifying DSM-5 AUDs in college students.
Introduction
Risky drinking practices among college students constitute as a significant public health concern. Prior research has indicated that rates of heavy and binge drinking among college students is higher compared to any other age group [1,2]. Of particular concern, during this critical developmental period, is that this level of alcohol involvement is associated with engagement in numerous alcoholrelated consequences that are unique to this important life transition (e.g. academic problems) [3-5]. An additional concern is that the prevalence of Alcohol Use Disorders (AUDs) also peaks during this time [6]. The onset of AUDs and continued heavy drinking during this critical period is associated with a more severe course of AUD in later adulthood, and if left undetected or untreated can lead to experiencing a greater number of and more consequential alcohol-related problems (e.g. health problems). This underscores the need to ensure that we can accurately screen for and identify the types of consequences endorsed among college students in order to intervene more effectively with them within our screening and brief intervention efforts. Moreover, a detailed assessment of the negative consequences arising from heavy alcohol use in college students may allow for a more accurate distinction between problem and nonproblem drinkers provide greater information about the risk for developing an AUD as well as identify specific consequences that are unique to those diagnosed with an AUD.
One of the most commonly used self-report measures of alcohol-related problems among college students is the Rutgers Alcohol Problem Index (RAPI) [5,7-10]. The RAPI is a 23-item screening measure that was originally validated for use with adolescents, and has been used extensively across various samples of adolescents since its inception [7]. During the past 15 years, however, several psychometric studies have validated the RAPI across diverse samples of college students documenting its reliability and validity among this at-risk population of drinkers [5,7-12]. Prior psychometric evaluation of the RAPI has documented its internal consistency reliability, factor structure, concurrent validity, predictive validity, convergent validity and test-rest reliability [5,8,12-14]. The RAPI has been used extensively in research involving college students to examine etiological processes of college drinking, develop cut-off scores to distinguish between problem and non-problem drinkers, assess the developmental trajectories of high-risk drinking, evaluate outcomes associated with intervention or treatment response, and in studies addressing the predictors of alcohol-related problems [11,15-18]. Collectively, prior research provides extensive empirical support for the RAPI as a brief, standardized screening measure for detecting alcohol-related problems in college students.
Despite its widespread use in college students, little attention has focused on examining the diagnostic performance of the RAPI in detecting AUDs. In one of the only evaluations of the diagnostic utility of the RAPI, among a sample of Finnish twins (n=597 pairs), RAPI scores at the age of 18 were found to be significant predictors of DSM-III alcohol dependence diagnoses in early adulthood (i.e. 25 years old) [8]. Receiving operating characteristic curves found a 74% probability that RAPI scores at 18 would be significantly higher among those with alcohol dependence than for those without a diagnosis at age 25. This study provides preliminary evidence of the RAPI in detecting AUDs; however, there are several gaps that warrant attention. Specifically, this study was conducted on a non-college sample, therefore little is still known about the diagnostic performance of the RAPI in detecting AUDs among college students. More importantly, there are currently no recommended cut-off scores on the RAPI that uniquely identify college students who are at-risk for developing an AUD. Given the robust associations between drinking problems and AUD diagnoses as well as the high rates of AUD among college students, it is critical that we ensure that our alcohol problem screening measures can accurately discriminate between those with and without an AUD [3-6]. An evaluation of the diagnostic precision of the RAPI in detecting AUDs among college students has the potential to enhance our collegiate screening and brief intervention efforts by ensuring it is a reliable and valid screening tool for identifying AUDs.
The primary taxonomic system used for diagnosing an AUD has been the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; APA 2000) [19]. Under this former system, it makes a hierarchical distinction between alcohol abuse and dependence (i.e. alcohol dependence criteria are more severe) with criteria sets to detect presence or absence of each disorder. Despite is widespread utility, several limitations have been associated with this binary classification approach [20-22]. As a result, the DSM-5 Substance Use Task Force has made the following changes to the AUD criteria in the DSM-5, which was released in 2013 [23]:
(a) Combine the abuse and dependence criteria into a singlediagnosis (> 2 criteria=an AUD);
(b) Create a severity qualifier that reflect a “minimal” (2 to 3 criteria endorsed), “moderate” (4 to 5 criteria endorsed) and “severe” (> 6 criteria endorsement) AUD;
(c) Add a craving criterion and remove the legal problemscriterion; and
(d) Rename the disorder to “Alcohol Use Disorder (AUD)”.
At present, research on the RAPI to screen for DSM-5 AUDs in college students has received no attention. Thus, it is critical that college drinking researchers and treatment providers’ move towards establishing cut-off thresholds on the RAPI and other alcohol screening measures based on the new DSM-5 AUD guidelines to ensure that our existing alcohol screening procedures are able to accurately identify and properly refer college students at-risk for an AUD.
In sum, the DSM-5 AUD criteria have been modified to reflect a single, continuous disorder. It is vital that we ensure that our existing alcohol screening tools maintain their accuracy in identifying AUDs. The RAPI is a widely used alcohol problem screening instrument that has been used extensively in diverse at-risk samples of college students. No studies have sought to answer important questions about the diagnostic performance of the RAPI in detecting DSM-5 AUDs. To address these critical questions, the aims of the current study were as follows:
a) To identify cut-off thresholds on the RAPI that maximizes sensitivity and specificity across college students with and without a DSM-5 AUD;
b) To determine whether RAPI cut-off scores vary by male and female college students; and
c) To evaluate the diagnostic performance of the RAPI in identifying college students with a DSM-5 AUD in comparison with other drinker classification groups including those with any DSM-IV AUD, low/high frequent drinkers and low/highquantity drinkers.
A detailed evaluation of the diagnostic performance of the RAPI in college students will provide recommendations for how to detect DSM-5 AUDs within our current alcohol screening practices.
Methods
Participants
The sample was collected at a large public university in the Northeastern part of the United States. Participants were recruited via:
1) Newspaper advertisements and paid $15.00 for their participation; and
2) Introductory Psychology courses were given course credit for their participation.
Prior to coming into the lab, each was screened via phone and was eligible to participant if they met the following requirements:
a) Undergraduate status;
b) Between the ages of 18 to 30; and
c) Engaged > 1 one binge drinking episode in the prior 90 days (> 5 for men and > 4 for women).
Upon entering the session, all participants provided informed consent and completed a 1 h anonymous battery of questionnaires. All procedures were approved by the university’s Institutional Review Board (IRB).
A total of 396 participants met eligibility requirements for the current study. Participants were between the ages of 18 to 30 (M=19.21; SD=1.29). The sample was diverse with respect to race and ethnicity with 59.8% (n=237) Caucasian, 6.6% (n=26) Hispanic, 8.3% (n=33) African-American, 19.9% (n=79) Asian, and 4% (n=16) were classified as other. With respect to class rank, 59.3% (n=235) were freshman, 20.2% (n=80) sophomores, 14.1% (n=56) juniors, and 5.6% (n=22) seniors. The majority were male (52%; n=206) and lived on campus (67.4%; n=267).
Measures
Alcohol and drug use: A modified Quantity/Frequency index (QFI) was used to collect participant alcohol use data in the prior 90 day period [24. Each participant estimated his/her frequency of consuming hard liquor, wine and beer (1=never; 7=everyday), and the quantity of alcohol they consumed per drinking occasion in the following three categories: hard liquor (1=never; 7=16 or more shots of liquor), wine (1=never; 7=16 or more 5-oz glasses of wine), and beer (1=never; 7=16 or more 12-oz cans/bottles). Separate frequency and quantity indices were created by summing the beer, liquor and wine items together. Principal components analyses indicated that each index was associated with a uni-dimensional structure accounting for approximately 51.4% and 47.6% of the common variance for the alcohol frequency and quantity indices, respectfully. Additional questions asked participants to report on their number of days consumed alcohol in the prior 90, greatest number of drinks consumed in a 24 h period, and the average number of standard drinks consumed on a typical weekday and weekend.
DSM-IV and DSM-5 AUD criteria: A self-administered modified version of the Composite International Diagnostic Interview-Substance Abuse Module (CIDI-SAM DSM-IV module) was used to collect DSM-IV and DSM-5 AUD diagnostic information with an additional question added to assess for the new DSM-5 craving criterion [25]. The DSM-5 craving question was included by asking participants the following: “During the past year, as a result of your alcohol use, did you have a strong desire or craving to drink?” as part of the data collection procedures, participants were asked to selfreport on the occurrence of each criterion within the past year. The CIDI-SAM DSM-IV diagnostic module has been used previously in prior research, which has indicated it to be both reliable and valid in college students [24,26].
Rutgers Alcohol Problem Index (RAPI): The Rutgers Alcohol Problem Index (23 items; RAPI) 7 was used to assess for the frequency of negative consequences from drinking in the prior year. Typically, RAPI items are scored on a Likert type scale, but for this study the items were dichotomized (0=did not occur; 1=did occur) and summed together to create an index of alcohol problem severity (Cronbach’s alpha=0.88). We dichotomized the RAPI items due to the inherent positive skew associated with the majority of the times in the sample as well as the fact that researchers often score the RAPI dichotomously to detect “presence” or “absence” of each consequence, and because prior research has indicated that a dichotomously scored RAPI is a reliable and valid measure in college students [9].
Classification of DSM-5 and DSM-IV AUDs
For the classification of the DSM-5 AUD diagnostic system, we used the guidelines set forth by DSM-5 Substance Use Task Force [19,23]. Participants who endorsed between 0 to only 1 criteria were classified as “no DSM-5 AUD”; and those who endorsed > 2 of any criteria were classified as “DSM-5 AUD+”. For the classification of DSM-IV AUD criteria, we used the guidelines set forth in the DSMIV- TR manual [19]. Participants who did not endorse any criteria or < 2 dependence criteria and no abuse criteria were classified as “no DSM-IV AUD”; those who endorsed between 1 to 4 abuse criteria and less than 3 dependence criteria were classified as “DSM-IV abuse/AB”; and those who endorsed 3 or more dependence criteria were classified as “DSM-IV dependent/AD”. For the current study, participants who were classified as either “DSM-IV abuse/AB” or “DSM-IV dependent/AD” were categorized as “any DSM-IV AUD” and the remaining participants were classified as “No DSM-IV AUD”.
Classification of alcohol quantity and frequency groups
For the current study, an alcohol quantity and frequency classification grouping variable was constructed using the QFI drinking data. A mean split for the alcohol quantity and frequency indices were applied to each of these constructed variables. For each alcohol classification grouping variable, participants were categorized into “high” and “low” drinker groups. Approximately, 51.8% (n=205) and 53.1% (n=210) were classified in the “high” drinker groups based on the alcohol frequency and quantity indices, respectively.
Data analytic plan
To determine optimal cut-off scores for distinguishing between those with and without a DSM-5 AUD, we calculated sensitivity, specificity, Positive Predictive Value (PPV), and Negative Predictive Value (NPV) across each potential RAPI score in the overall sample and separately for males and females. Due to lower numbers of endorsement at the higher RAPI cut-off scores, our analyses focused on RAPI cut-off scores between 1 to 14 (RAPI scores range from 0 to 23). Sensitivity is the true positive rate and reflects the percentage of all individuals with active DSM-5 AUD symptomatology who score above a threshold score on the RAPI. Specificity is the true negative rate and reflects the percentage of individuals who do not meet DSM-5 AUD diagnostic criteria and score below a threshold score on the RAPI. The Positive Predictive Value (PPV) is the probability that participants with a positive screening test at that specific RAPI cutoff score have a DSM-5 AUD diagnosis. Negative Predictive Value (NPV) is the probability that participants with a negative screening (i.e. score below the RAPI cut-off score) tests do not have a DSM-5 AUD diagnosis. Because sensitivity and specificity does not always provide a clear distinction in the identification of an optimal cut-off score, Youden index (J) was calculated by the following equation: J = (Sensitivity + Specificity) - 1. Youden index score ranges from 0 to 1 with a score of 1 indicating that the RAPI cut-off has perfect diagnostic predictability and a score close to 0 indicating no diagnostic predictability. The cut-off score with the highest J value is selected as the most optimal, but the decision is contingent upon finding a good balance between sensitivity and specificity. The identification of an optimal cut-off score typically maximizes sensitivity over specificity.
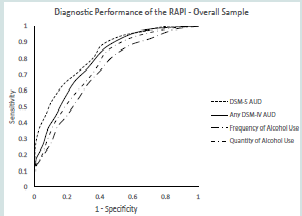
Receiving Operating Characteristic (ROC) curve analyses were used to evaluate the performance of the RAPI in discriminating across the following reference standards: DSM-5 AUD, any DSM-IV AUD, high/low frequent drinkers and high/low quantity drinkers. ROC curves plotted sensitivity (Y-axis) vs. 1 - Specificity (X-axis) for each reference standard. Curves that peak toward the upper left hand corner of a ROC graph indicate that the RAPI is a strong screening test for that specific reference standard. We also calculated Areas Under Receiving Operating Characteristic Curves (AUROCs), along with the 95% Confidence Intervals (95% CIs), to determine which referent standard provides the most optimal combination of sensitivity and specificity. Typically, the higher the AUROC, the stronger the performance of the RAPI for distinguishing between a selected reference standard with scores ranging between 0.70 or higher considered good to excellent. We conducted ROC and AUROC analyses across the overall sample and separately for males and females.
Results
Alcohol use characteristics
Participants reported consuming alcohol, on average, 17 days (M=17.29; SD=14.46) out of the prior 90 days. Approximately, 86.7% (n=344) of the sample reported binge drinking in the prior two weeks of study onset. The typical number of drinks consumed per weekday was 2.94 (SD=2.73) and 5.84 (SD=3.93) per day on the weekend. On average, the greatest amount consumed within a 24 h period was 9.67 (SD=5.68) standard drinks.
Classification of DSM-IV and DSM-5 AUD drinker groups
Based on the DSM-5 AUD classification scheme, approximately 50% (n=198) and 50% (n=198) were classified as “no DSM-5 AUD” and “DSM-5 AUD+”, respectfully. With respect to the classification rates of DSM-IV AUDs in the sample, 16.7% (n=66) and 23.2% (n=92) were classified as alcohol abuse and alcohol dependent.
RAPI characteristics
The overall sample reported, on average, endorsing a total of 6 (M=5.91; SD=4.42) negative consequences from drinking on the RAPI. The most frequently endorsed RAPI items were as follows:
1) “Had a bad time” (52.5; n=208);
2) “Not able to do your homework or study for a test” (48.7%; n=193);
3) “Neglected your responsibilities” (45.2%; n=179);
4) “Felt that you need more alcohol than you used to in order to get the same effect” (41.4%; n=164); and
5) “Had a fight, argument or bad feeling with a friend” (39.9%; n=155).
RAPI diagnostic performance results
Overall sample: The AUROC value for those classified with a DSM-5 AUD was 0.828 (SE=0.20; 95% CI, 0.789-0.867). Among those classified with a DSM-IV AUD, the AUROC value was slightly lower (0.791; SE= 0.022; 95% CI, 0.748-0.835). The AUROC values for the alcohol quantity and frequency groups were 0.758 (SE=0.024; 95 CI, 0.711-0.805) and 0.719 (SE=0.025; 95 CI, 0.669-0.769), respectfully. The AUROC value for the alcohol quantity group was higher than the value for the alcohol frequency group, but neither was higher than the values for either DSM-5 AUD status or DSM-IV AUD status. All AUROC values were significantly greater than the chance value of 0.50 indicating that the RAPI has reasonably good discrimination across several pertinent alcohol use risk groups. This is confirmed by Figure 1, which displays the ROC for each of our alcohol reference groups. The DSM-5 AUD reference group ROC had the highest peak followed by the DSM-IV AUD reference group, whereas the alcohol quantity and frequency groups were associated with significantly lower ROCs.
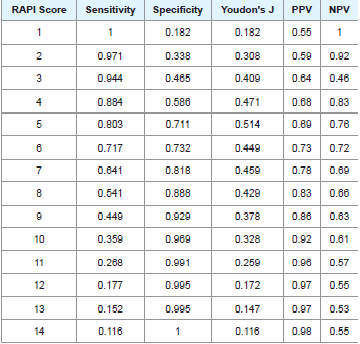
To determine the most optimal cut-off score on the RAPI that distinguish between those with and without a DSM-5 AUD, we calculated and evaluated sensitivity, specificity, PPV, NPV and Youden index score across each potential RAPI cut-off score (Table 1 displays these values across each RAPI cut-off score). Using DSM-5 AUD status as the primary reference group, the sensitivity and specificity values across the cut-off scores ranged from 0.116 to 0.971 and 0.182 to 0.995, respectively. A RAPI cut-off score of 5 had the highest Youden’s J index score, which was equal to 0.514 with reasonably high sensitivity and specificity values of 0.803 and 0.711, respectively. In addition, the PPV and NPV values at the RAPI cut-off score of 5 were 0.69 and 0.76.
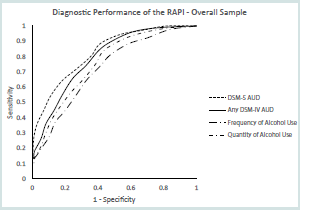
Males: The AUROC value for DSM-5 AUD status among males was 0.822 (SE=0.028; 95 CIs, 0.767-0.878). With respect to those classified with any DSM-IV AUD, the AUROC value was lower (0.737; SE=0.034; 95% CIs, 0.669-0.804). The AUROC values for the alcohol quantity and frequency classification groups were 0.724 (SE=0.037; 95% CIs, 0.652-0.796) and 0.646 (SE=0.038; 95% CIs, 0.571-0.722). Similar to the AUROC analysis in the overall sample, the AUROC value for the alcohol quantity group was higher than the value for the alcohol frequency group, whereas both values were lower than the those for the DSM-5 AUD and DSM-IV AUD reference groups. All AUROC values in the were significantly greater than the chance value of 0.50 indicating that the RAPI has reasonably good discrimination across several pertinent alcohol use risk groups among male college students. This is confirmed by Figure 2, which displays the ROC for each of our alcohol reference groups. The DSM-5 AUD reference group ROC had the highest peak followed by the DSM-IV AUD reference group, whereas the alcohol quantity and frequency groups were associated with significantly lower ROCs.
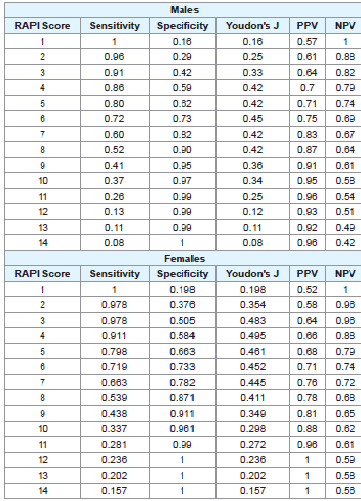
The sensitivity, specificity, PPV, NPV and Youdon’s J index scores across each RAPI cut-off score among male college students is displayed in Table 2. Using the DSM-5 AUD status as the primary reference standard, the sensitivity and specificity values across the cut-off scores ranged from 0.116 to 0.971 and 0.182 to 0.995, respectively. A RAPI score of 6 had the highest Youden’s J index score, which was equal to 0.45 with reasonably high sensitivity and specificity values ranging from 0.73 to 0.72. Along these lines, the values for PPV and NPV at a RAPI cut-off score of 6 were 0.75 and 0.69, respectively.
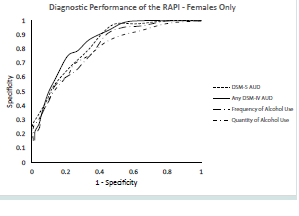
Females: The AUROC value for DSM-5 AUD status among females was 0.833 (SE=0.028; 95 CIs, 0.778-0.888). With respect to those classified with any DSM-IV AUD, the AUROC value was slightly higher (0.847; SE=0.027; 95% CIs, 0.794-0.901). The AUROC values for the alcohol quantity and frequency classification groups were 0.803 (SE=0.031; 95% CIs, 0.742-0.863) and 0.792 (SE=0.032; 95% CIs, 0.729-0.855). Similar to the AUROC analysis in the overall sample, the AUROC value for the alcohol quantity group was higher than the value for the alcohol frequency group, whereas both values were lower than those for the DSM-5 AUD and DSM-IV AUD reference groups. In contrast to the male only sample, the AUROC values for the alcohol reference groups were higher indicating slightly better diagnostic performance of the RAPI among females. All AUROC values in the were significantly greater than the chance value of 0.50 indicating that the RAPI has reasonably good discrimination across several pertinent alcohol use risk groups among female college students. This is confirmed by Figure 3, which displays the ROC for each of our alcohol reference groups. The DSM-IV AUD reference group ROC had the highest peak followed by the DSM-5 AUD reference group, whereas the alcohol quantity and frequency groups were associated with significantly lower ROCs.
The sensitivity, specificity, PPV, NPV and Youdon’s J index scores across each RAPI cut-off score among female college students is displayed in Table 2. Using the DSM-5 AUD status as the primary reference standard, the sensitivity and specificity values across the cutoff scores ranged from 0.157 to 0.978 and 0.198 to 0.99, respectively. A RAPI score of 4 had the highest Youden’s J index score, which was equal to 0.494 with reasonably high sensitivity and specificity values ranging from 0.911 to 0.584. Along these lines, the values for PPV and NPV at a cut-off score of 4 were 0.66 and 0.88, respectively.
Discussion
This is the first study to examine the diagnostic performance of the RAPI in detecting DSM-5 AUDs in a sample of college students. The overall performance of the RAPI was high and adequate (AUC=0.828) in classifying college students with DSM-5 AUDs. This finding is consistent with prior research which found a high AUC for the RAPI in predicting alcohol use dependence diagnoses in a sample of 18 year Finnish twins [8]. This study also found that an overall RAPI cut-off score of > 5 provided a reasonable balance of sensitivity and specificity and maximized Youden’s J index in the detection of DSM-5 AUDs. These findings highlight the need to continue toreplicate and determine the stability of the current study findings across diverse samples of at-risk college students.
Findings from this study revealed gender specific RAPI cut-off scores in detecting DSM-5 AUDs among college students. Among the current sample, RAPI cut-off scores of > 4 for females and > 6 for males provided the most optimal balance between sensitivity and specificity and provide the highest Youden’s J index in classifying college students with a DSM-5 AUD. This finding highlights that the cut-off scores on the RAPI necessary to detect DSM-5 AUDs in college students are lower for women in comparison to men. Prior research using other alcohol screening tools (e.g. AUDIT-C) have consistently documented lower cut-off scores among women in comparison to men in classifying DSM-IV and DSM-5 AUDs across diverse sample of drinkers [27-29]. The lower cut-off thresholds on the RAPI among women in comparison to men are likely attributed to several factors. For example, it is well documented that women have unique biological characteristics such that women develop a higher BAC in comparison to men after consuming the same amount of alcohol. Additionally, women are more likely to be susceptible to the toxic effects of alcohol and develop health problems related to alcohol consumption earlier (e.g. liver disease) [30,31]. Based on this evidence, the current study findings provide support for using lower RAPI cut-off scores in females relative to males in college for detecting DSM-5 AUDs.
Several notable findings from this study were that the RAPI performed slightly better (although not statistically significantly different from one another) in detecting DSM-5 AUDs in comparison to DSM-IV AUDs, and performed most optimally in detecting DSM-5 AUDs in comparison to alcohol use (both quantity and frequency). The optimal performance of the RAPI in screening for DSM-5 AUDs in comparison to DSM-IV AUDs may be partially explained, in part, via the merging of the AUD together into a single diagnosis. Under the former DSM-IV AUD system, individuals who endorsed between 1 to 2 dependence criteria and no abuse criteria, do not receive a formal diagnosis, despite closely resembling those with an alcohol abuse diagnosis across pertinent alcohol use risk factors [32-34]. It is possible, therefore, that the merging of the DSM-5 AUD criteria may have resulted in better detection of the RAPI by providing greater coverage of DSM-IV subthreshold drinkers (i.e. diagnostic orphans) under the new system [32-34]. The lower AUC values associated with the alcohol frequency and quantity groups in comparison to the DSM-5 and DSM-IV AUD groups is likely explained, in part, by the fact that correlations between alcohol-related problem measures, such as the RAPI and DSM-5 AUD criteria, reflect the same construct of alcohol problem severity and are consistently associated with higher correlations in comparison to measures of alcohol use, which have been shown to be associated with slightly lower correlations. Therefore, study findings indicate that the RAPI is more optimal in detecting AUDs in comparison to alcohol consumption among college students.
The current study findings provide several avenues for future exploration in screening for DSM-5 AUDs in college students. First, the stability of derived study findings is not known. Continued research in other at-risk samples of college students is necessary to replicate and ensure that the current findings can be generalized to diverse samples of drinkers in college. Next, the diagnostic performance of the RAPI in detecting the DSM-5 AUD severity groups (mild, moderate, severe) was not examined in this study. Future research should evaluate the performance of the RAPI in screening for the DSM-5 AUD severity groups as well as develop established cut-off scores on the RAPI that may classify college students based on their AUD severity. Lastly, this study did not determine if the diagnostic performance of the RAPI in detecting DSM-5 AUDs among college students varies across select demographic characteristics (e.g. race/ ethnicity; college rank). A detailed evaluation of the extent to which the diagnostic performance of the RAPI varies across demographic factors has the potential to assist in tailoring our alcohol screening initiatives for detecting DSM-5 AUDs to specific sub-groups of college students.
There were several limitations associated with the current study. First, the primary outcomes of interest were based on participant self-reports, which can be impacted by recall biases. Several methodological procedures, such as assurances of anonymity and the use of psychometrically sound questionnaires, were incorporated into the study to enhance response accuracy, thereby reducing this concern [35]. Next, the DSM-5 AUD diagnostic criteria were collected via selfreport and not through a more rigorous clinical interview, which is considered the “gold standard” for collecting diagnostic information [26]. That said, the items used to assess for DSM-5 AUD criteria were adapted from a prior clinical interview [25]. Moreover, the correlations between the sum of DSM-5 AUD criteria and pertinent alcohol use variables in this sample were positive and in the moderate to high range providing support to the validity of the diagnostic questionnaire administered. Lastly, a convenience sample of college students (i.e. mainly recruited via Introductory Psychology courses) was used in this study potentially impacting the generalizability of the study findings. Concerns about the representativeness may be allayed because drinking rates reported in the current sample are similar to those from other studies of alcohol use among college students [1,2].
In sum, this is one of the first studies to evaluate the diagnostic performance of the RAPI in detecting DSM-5 AUDs in a sample of non-treatment seeking college students. This study provides preliminary support for the RAPI as a valid alcohol problems screening instrument in classifying college students with DSM-5 AUDs. Findings indicate also that the RAPI has a high degree of diagnostic precision in screening for DSM-5 AUDs across males and females in college, and suggests that different gender-specific RAPI cut-off threshold be used to detect DSM-5 AUDs. Given the elevated rates of heavy drinking and alcohol problems in college students, it is vital that we can ensure that our alcohol screening measures maintain their accuracy in detecting DSM-5 AUDs within our collegiate alcohol screening and brief intervention protocols. The detection of DSM-5 AUDs in college students using the RAPI is a necessary first step towards enhancing our alcohol screening efforts under the new diagnostic system.
Declaration of Interest
The contents of this manuscript only reflect the views of the authors and not those of the National Institute on Alcohol Abuse and Alcoholism (NIAAA) or the National Institutes of Health. The author(s) report no conflicts of interest influencing results of derived study findings. Parts of this manuscript have been presented at the Research Society on Alcoholism’s annual conference.
Acknowledgement
The current study was funded from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) via grant #T-32 AA07569-17. The author(s) would like to thank Dr. Amy Cohn (Research Scientist at the Legacy Foundation and Truth Initiative) for her helpful feedback and comments.
References
- Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, et al. (2002) Trends in college binge drinking during a period of increased prevention efforts. Findings from 4 Harvard School of Public Health college alcohol study surveys: 1993-2001. J Am Coll Health 50: 203-217.
- Wechsler H, Lee JE, Kuo M, Lee H (2000) College binge drinking in the 1990s: a continuing problem. Results of the Harvard school of public health 1999 college alcohol study. J Am Coll Health 48: 199-210.
- Beck KH, Arria AM, Calderia KM, Vincent KB, O'Grady KE, et al. (2008) Social context of drinking and alcohol problems among college students. Am J Health Behav 32: 420-430.
- Kahler CW, Strong DR, Read JP, Palfai TP, Wood MD (2004) Mapping the continuum of alcohol problems in college students: a Rasch model analysis. Psychol Addict Behav 18: 322-333.
- Neal DJ, Corbin WR, Fromme K (2006) Measurement of alcohol-related consequences among high school and college students: application of item response models to the Rutgers Alcohol Problem Index. Psychol Assess 18: 402-414.
- Knight JR, Wechsler H, Kuo M, Seibring M, Weitzman ER, et al. (2002) Alcohol abuse and dependence among U.S. college students. J Stud Alcohol 63: 263-270.
- White HR, Labouvie EW (1989) Towards the assessment of adolescent problem drinking. J Stud Alcohol 50: 30-37.
- Dick DM, Aliev F, Viken R, Kaprio J, Rose RJ (2011) Rutgers Alcohol Problem Index scores at age 18 predict alcohol dependence diagnoses 7 years later. Alcohol Clin Exp Res 35: 1011-1014.
- Martens MP, Neighbors C, Dams-O'Connor K, Lee CM, Larimer ME (2007) The factor structure of a dichotomously scored Rutgers Alcohol Problem Index. J Stud Alcohol Drugs 68: 597-606.
- Light LS, McCoy TP, Thompson MP, Spitler HD, Sutfin EL, et al. (2011) Modeling the Rutgers Alcohol Problem Index (RAPI): a comparison of statistical methods. Addict Res Theory 19: 510-518.
- Noel M, O’Connor RM, Boudreau B, Mushquash CJ, Comeau MN, et al. (2010) The Rutgers Alcohol Problem Index (RAPI): a comparison of cut-points in first nations Mi’kmaq and non-aboriginal adolescents in rural Nova Scotia. Int J Ment Health Addict 8: 336-350.
- Cohn AM, Hagman BT, Graff FS, Noel NE (2011) Modeling the severity of drinking consequences in first-year college women: an item response theory analysis of the Rutgers Alcohol Problem Index. J Stud Alcohol Drugs 72: 981-990.
- Earleywine M, LaBrie JW, Pedersen ER (2008) A brief Rutgers Alcohol Problem Index with less potential for bias. Addict Behav 33: 1249-1253.
- Miller ET, Neal DJ, Roberts LJ, Baer JS, Cressler SO, et al. (2002) Test-retest reliability of alcohol measures: is there a difference between internet-based assessment and traditional methods? Psychol Addict Behav 16: 56-63.
- Lewis MA, Neighbors C (2004) Gender-specific misperceptions of college student drinking norms. Psychol Addict Behav 18: 334-339.
- White HR, Labouvie EW (2000) Longitudinal trends in problem drinking as measured by the Rutgers Alcohol Problem Index. Alcohol Clin Exp Res 24: 76A.
- Borsari B, Carey KB (2005) Two brief alcohol interventions for mandated college students. Psychol Addict Behav 19: 296-302.
- Orona JA, Blume AW, Morera OF, Perez S (2007) Examining drinking consequences and reasons for drinking in a bilingual college sample. Hispanic J Behav Sci 29: 101-115.
- American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, (4thedn). Washington, USA.
- Hasin DS, Fenton MC, Beseler C, Park JY, Wall MM (2012) Analyses related to the development of DSM-5 criteria for substance related disorders: 2. Proposed DSM-5 criteria for alcohol, cannabis, cocaine and heroin disorders in 663 substance abuse patients. Drug Alcohol Depend 122: 28-37.
- Hasin S, Grant BF (2004) The co-occurrence of DSM-IV alcohol abuse in DSM-IV alcohol dependence: results of the National Epidemiologic Survey on alcohol and related conditions on heterogeneity that differ by population subgroup. Arch Gen Psychiatry 61: 891-896.
- Hasin D, Hatzenbuehler ML, Keyes K, Ogbum E (2006) Substance use disorders: diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV) and International Classification of Diseases, tenth edition (ICD-10). Addiction 101 (Suppl 1): 59-75.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, (5thedn), Arlington, USA.
- Hagman BT, Cohn AM (2011) Toward DSM-V: mapping the alcohol use disorder continuum in college students. Drug Alcohol Depend 118: 202-208.
- Robins LN, Cottler LB, Babor T (1995) CIDI-substance abuse module. St. Louis, Washington University School of Medicine, USA.
- Clements R (1998) A critical evaluation of several alcohol screening instruments using the CIDI-SAM as a criterion measure. Alcohol Clin Exp Res 22: 985-993.
- Hagman BT (2015) Toward efficient screening for DSM-5 alcohol use disorders in college students: performance of the Audit-C. Addict Disord Their Treat 14: 1-15.
- Hagman BT (2016) Performance of the Audit in detecting DSM-5 alcohol use disorders in college students. Subst Use Misuse 51: 1521-1528.
- Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA (1998) The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med 158: 1789-1795.
- Bradley KA, Badrinath S, Bush K, Boyd-Wickizer J, Anawalt B (1998) Medical risks for women who drink alcohol. J Gen Intern Med 13: 627-639.
- Brienza RS, Stein MD (2002) Alcohol use disorders in primary care: do gender-specific differences exist? J Gen Intern Med 17: 387-397.
- Hagman BT, Cohn AM (2012) Drinking correlates of DSM-IV alcohol use disorder diagnostic orphans in college students. Am J Addict 21: 233-242.
- Harford TC, Yi HY, Grant BF (2010) The five-year diagnostic utility of “diagnostic orphans” for alcohol use disorders in a national sample of young adults. J Stud Alcohol Drugs 71: 410-417.
- Eng MY, Schuckit MA, Smith TL (2002) A five-year prospective study of diagnostic orphans for alcohol use disorders. J Stud Alcohol 64: 227-234.
- Babor TF, Del Boca FK (1992) Just the facts: enhancing the measurement of alcohol consumption using self-report methods. In: Litton RZ, Allen JP (Eds), Measuring alcohol consumption: psychosocial and biochemical methods. Humana Press, Springer, New York, USA, pp. 3-19.