
Journal of Oral Biology
Download PDF
Research Article
*Address for Correspondence: Dr. Ahmed Elkhaweldi, Former Resident, New York University College of Dentistry, 36-04 31st Avenue, Apt #2B, Astoria, New York, USA, E-mail: ae815@nyu.edu
Citation: Elkhaweldi A, Lee DH, Wang W, Cho SC. The Survival Rate of RBM Surface versus SLA Surface in Geometrically Identical Implant Design. J Oral Bio. 2014;1(1): 8.
Copyright © 2014 Elkhaweldi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 1
Submission: 08 October 2014 | Accepted: 19 December 2014 | Published: 22 December 2014



 Patient who had uncontrolled systemic disease were excluded from this study. All the patients included in this study were periodontal disease free. The bone quality was considered poor when the patient had type IV bone (Zarb and lekholm) and had less than 15Ncm primary stability. All of the implants were surgically placed by the same surgeon (SC), while another restorative dentist restored them.
Patient who had uncontrolled systemic disease were excluded from this study. All the patients included in this study were periodontal disease free. The bone quality was considered poor when the patient had type IV bone (Zarb and lekholm) and had less than 15Ncm primary stability. All of the implants were surgically placed by the same surgeon (SC), while another restorative dentist restored them.
 Third, we determined the magnitude of the effect of the implant surface type on implant failures by using logistic regression analyses in which implant failure was the dependent variable and implant surface type and the relevant covariates (as defined above) were the independent variables. 5% level of significance was used.
Third, we determined the magnitude of the effect of the implant surface type on implant failures by using logistic regression analyses in which implant failure was the dependent variable and implant surface type and the relevant covariates (as defined above) were the independent variables. 5% level of significance was used.

 Overall, considering the two groups of either RBM or SLA surfaced implants, a total of nine implants failed in 6 patients achieving an overall survival rate of 96.7%. The first group included 167 RBM implants while the second group included 113 SLA implants. Only one implant from the SLA group was lost compared to eight implants that failed in the RBM group. Thus, the SLA implant group’s survival rate was 99.1% while that of RBM implants group’s was 95.2% (Tables 5a and b).
Overall, considering the two groups of either RBM or SLA surfaced implants, a total of nine implants failed in 6 patients achieving an overall survival rate of 96.7%. The first group included 167 RBM implants while the second group included 113 SLA implants. Only one implant from the SLA group was lost compared to eight implants that failed in the RBM group. Thus, the SLA implant group’s survival rate was 99.1% while that of RBM implants group’s was 95.2% (Tables 5a and b).

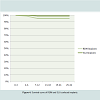
 Implant failure in the two surface groups: When we compared implants with SLA and implants with RBM surface, mean failed implants tended to be lower in the SLA group compared to RBM group (0.01 vs. 0.05; p=0.07). The time of follow up, implant diameter and the number of implants placed in diabetes subjects were different between the two two groups. To account for these variables, we performed ANCOVA with these parameters as covariates. The adjusted means were statistically significant (p=0.039). These results showed that the mean failure is lower in SLA compared to RBM group and diabetes, smoking and follow-up time did not account for this difference (Figure 4).
Implant failure in the two surface groups: When we compared implants with SLA and implants with RBM surface, mean failed implants tended to be lower in the SLA group compared to RBM group (0.01 vs. 0.05; p=0.07). The time of follow up, implant diameter and the number of implants placed in diabetes subjects were different between the two two groups. To account for these variables, we performed ANCOVA with these parameters as covariates. The adjusted means were statistically significant (p=0.039). These results showed that the mean failure is lower in SLA compared to RBM group and diabetes, smoking and follow-up time did not account for this difference (Figure 4).
 Using logistic regression, we estimated the magnitude of the implant surface effect on predicting implant failures. Since the covariates age, gender, smoking, anatomical area, implant length did not differ between the two groups, they were not included in the final model. However, diabetes and time to follow-up were statistically significant difference between the two groups and therefore were included in the models. As shown in Table 3, three models were constructed. In our crude analysis the implant surface type was a significant predictor of the implant failure but only at a trend level (OR=5.64; p=0.11). When in sequential models the follow up time and diabetes were added to the models the OR became even stronger (OR=6.40 and 6.52 respectively) suggesting that these parameters did not change the surface effect on increasing implant failure. Pertaining to our results we observed a significant effect of follow-up time on the implant failure independent of the surface effect. Our results showed that the follow up time was a significant predictor of the implant failure: with each year increase in the follow up there was a significant odds of not-failures. In other words, as the time passed the odds of failures decreased (p=0.009).
Using logistic regression, we estimated the magnitude of the implant surface effect on predicting implant failures. Since the covariates age, gender, smoking, anatomical area, implant length did not differ between the two groups, they were not included in the final model. However, diabetes and time to follow-up were statistically significant difference between the two groups and therefore were included in the models. As shown in Table 3, three models were constructed. In our crude analysis the implant surface type was a significant predictor of the implant failure but only at a trend level (OR=5.64; p=0.11). When in sequential models the follow up time and diabetes were added to the models the OR became even stronger (OR=6.40 and 6.52 respectively) suggesting that these parameters did not change the surface effect on increasing implant failure. Pertaining to our results we observed a significant effect of follow-up time on the implant failure independent of the surface effect. Our results showed that the follow up time was a significant predictor of the implant failure: with each year increase in the follow up there was a significant odds of not-failures. In other words, as the time passed the odds of failures decreased (p=0.009).
The Survival Rate of RBM Surface versus SLA Surface in Geometrically Identical Implant Design
Elkhaweldi Ahmed1*, Lee Dong Hyun2, Wang Wendy CW3 and Cho Sang Choon4
- 1New York University College of Dentistry, New York, USA
- 2Englewood Cliffs, New Jersey, USA
- 3New York University College of Dentistry, New York, USA
- 4Department of Periodontology and Implant Dentistry, New York University College of Dentistry, New York, USA
*Address for Correspondence: Dr. Ahmed Elkhaweldi, Former Resident, New York University College of Dentistry, 36-04 31st Avenue, Apt #2B, Astoria, New York, USA, E-mail: ae815@nyu.edu
Citation: Elkhaweldi A, Lee DH, Wang W, Cho SC. The Survival Rate of RBM Surface versus SLA Surface in Geometrically Identical Implant Design. J Oral Bio. 2014;1(1): 8.
Copyright © 2014 Elkhaweldi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Oral Biology | ISSN: 2377-987X | Volume: 2, Issue: 1
Submission: 08 October 2014 | Accepted: 19 December 2014 | Published: 22 December 2014
Abstract
Introduction: Although many studies have been conducted to compare the survival rate of dental implants with different degree of roughness, there is scarcity of studies that compare the survival rate of implants with two different surfaces and have geometrically identical body design.Purpose: The purpose of this study was to evaluate and discuss the difference in survival rates between two geometrically identical implant groups with two different surfaces to help understand the effect of implant surface roughness on their survival rate.
Materials and methods: The data in this study were obtained retrospectively from the consecutive analysis of anonymous database at New York University College of Dentistry. The clinical records for 161 patients (102 males, and 59 females) were gathered. The study included 280 implants of the same identical geometrical design and had either RBM or SLA surface. The follow up time since the implants were restored ranged from 4 to 32 months (average 18 months).
Results: A total of nine implants have failed in six patients. The overall survival rate of the 280 implants was 96.7%. The first group included 167 RBM implants while the second group included 113 SLA implants. Only one implant from the SLA group was lost compared to eight implants that have failed from the RBM group. The SLA implants group had higher survival rate of 99.1% while RBM implants group was found to have a survival rate of 95.2%.
Conclusions: Within the limitation of this study, geometrically identical implants with either RBM or SLA surface have a very comparable survival rates at least in the short term. However, the SLA surface seems to be superior in the posterior maxilla with poor bone. Since the overall failure rate is very low, more studies with higher subjects number and longer follow up are needed.
Introduction
The early experimental studies in the field of implant dentistry suggested that an inert titanium implant could be surgically inserted in an edentulous alveolar ridge. Once the implant is in place, sequence of soft and hard tissue healing around it will follow. Eventually the implant can be utilized in anchoring dental prostheses [1]. Branemark group was the first to report that titanium implants could be incorporated within the bone through oxide layer and as a result, the two could not be disconnected without fracture. This phenomenon has been referred to as osseointegration or osteointegration, which mandate a direct bone-to-implant contact with absence of fibrous tissue encapsulation [2].Ever since, the bone-to-implant interface has been studied extensively with great emphasis on the implant surface characteristics. On one hand, it is believed that osseointegration between bone and titanium implants can be achieved and maintained for a long period oftime regardless of their surface characteristics [3]. On the other hand, the majority of in-vivo and in-vitro studies found that an implant surface with some degree of roughness has a better and an accelerated process of healing toward achieving osseointegration [4]. It has been shown that there is a positive relationship between the degree of roughness and the speed of osseointegration. One study showed that implants with surface roughness (Sa) ranging between 0.5-1 μm have a weaker bone response compared to implants that have (Sa) ranging between 1-2 μm [5]. One systematic review concluded that smooth (Sa 0.5 μm) and minimally rough (Sa0.5–1 μm) surfaces show reduced and slower bone responses than rougher surfaces. Interestingly, moderately rough (Sa 1–2 μm) surfaces showed better bone responses than highly rough surfaces (Sa >2 μm) [6]. It was previously shown that implants with rougher surface have more bone-to-implant contact at period 3-6 weeks than implants with less rough surface. In addition to that, a recent in vitro study found that rough surfaces (1-2 μm) are more preferable by osteoblasts as they increase the gene expression for Cbfα1 mRNA of osteoblast. Osteoblast also showed an enhanced adherence and propagation on rough surfaces compared to machined surface implants [7,8].
Different techniques have been utilized to alter the surface topography of dental implants. These techniques are usually applying either additive or subtractive concepts. One of the early used techniques is the Titanium Plasma Spray (TPS) which is an additive technique resulting in an increase of the surface area up to six times [9]. Hydroxyapatite (HA) plasma spray is also one of the early additive techniques developed for coating dental implants with biomaterials to change their surface characteristics. The early results of this technique were very promising as it enhanced the osseointegration of dental implants, but follow up studies showed that the use of plasmasprayed HA to coat dental implants has increased the clinical failure which was attributed to the delamination of the thick HA layer and to the uncontrolled rate of dissolution of deposited phases [10,11]. The additive surfaces became less preferred by clinicians than the subtractive surfaces. Long term follow up studies for these surfaces have shown increased risk of peri-implantitis and eventually led to a decline in their survival rate [6,12]. TPS surfaces have also shown poorresponse to treatment of peri-implantitis. Consequently, subtractive surfaces like Sand blasted and Acid etched (SLA), Resorbable Blast Media (RBM), and Dual Acid Etching (DAE), which have moderate roughness, became more popular [13].
Currently, the two major subtractive surfaces in clinical use are the SLA surface and the RBM surface [9]. SLA surface is created first by sandblasting with large grit particles then followed by acid etching to remove the remaining particles and further increase the roughness. The SLA surface has surface average roughness (Sa 1.78 μm) [9,14]. One study that looked at the survival rate of SLA implants found that after 10 years period of follow up, these implants had 98% survival rate [15]. Simone et al. also reported survival rate for SLA surfaced implants of 82.94% after a follow up period of 10-16 years [16]. Resorbable blast media surface (RBM) is formed through propelling resorbable coarse bioceramics (calcium phosphate) particles on titanium metal substrate followed by passivation process aiming to increase the level of roughness and enhance the osseointegration capability of the implant. One of the advantages of this technique is gained via the use of calcium phosphate particles that eliminates the risk of leaving contaminating debris after blasting. Leaving contaminated surface is considered a common drawback for using other less biocompatible blasting materials. RBM surface possesses average roughness around 1.5 μm [17,18]. In one animal study, RBM surface had a higher bone to implant contact after 90 days than either of TPS, HA coated, and smooth surface implants [19]. As far as RBM surface survival rate is a concern, studies have reported comparable survival rate of 95.37% after 7 years of follow up period [20].
With regard to comparing the effect of the implant surface characteristics on the survival rate, the literature is rich with large numbers of studies investigating this issue but all of the previously studies cited in this article have compared different implant surfaces on different geometrical design. For example, Al Nawas et al. compared the survival rate of turned surfaced implants from Nobel Biocare to double acid etched surfaced implants from Biomet 3i. After periods of 49 months follow up, no difference in the survival rate has been found between the two surfaces [21]. Another similar study by Khang et al. that compared the survival rate of machined surfaced implants to double acid etched surfaced implants found that the latter had a 9% higher survival rate of 95% [22].
According to the author’s knowledge, there is a scarcity of clinical studies that compare the survival rates of two surfaces with the same exact body design. One study by Li et al. compared the removal torque and the bone response of two identical implants with either SLA surface, machined surface, or dual acid etched surface and found that SLA surface achieved a better bone anchorage and had more than 5% higher stiffness of the removal torque test [23]. Therefore, the aim of this study was to evaluate and discuss the survival rate of SLA surface to RBM surface for implants with identical geometrical design.
Materials and Methods
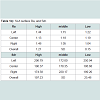
The data in this study were obtained retrospectively from the consecutive analysis of anonymous database at New York University College of Dentistry. The clinical records for 161 patients (102 males, and 59 females) were gathered. These patients have received a total of 280 implants all of which had the same body design with diameter ranging from 4.1 mm to 4.8 mm and length ranging of 9 to 13 mm (average 11 mm). The age of the patients in this study ranged from 21 to 81 (average 55.3 years). Implants were placed in the period between March 2012 to February 2014. The study included 167 implants with RBM surface and 113 implants with SLA surface. All of the survived implants are restored and in function at the time of this study. The follow up time since the implants were restored ranged from 4 to 32 months.The study included only patients who had received implants of the same identical geometrical design and had either RBM or SLA surface (EBI Inc., Kyungsan, South Korea), (Figures 1 and 2). The surface roughness parameters for each surface represented in Ra and Sdr are shown in ( Tables 1a and 1b).

Figure 1: Two geometrically identical implants, 4.1 mm X 11 mm, the RBM surfaced implant on the left and the SLA surfaced implant on the right.
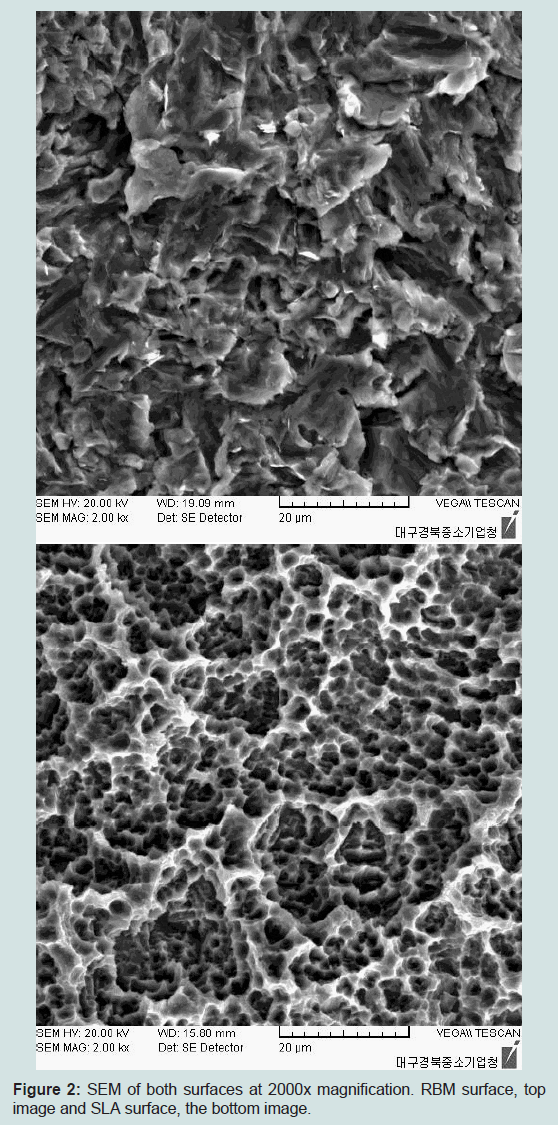
Figure 2: SEM of both surfaces at 2000x magnification. RBM surface, top image and SLA surface, the bottom image.
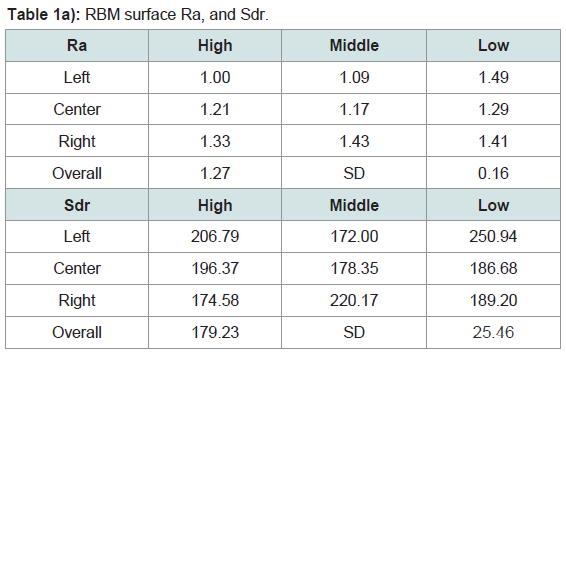
Table 1a: RBM surface Ra, and Sdr.
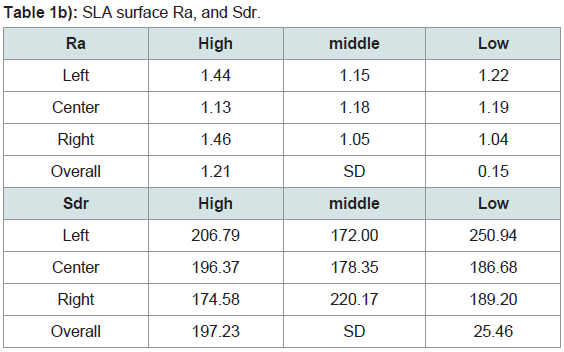
Table 1b: SLA surface Ra, and Sdr.
Statistical Analysis
Statistical analyses were performed using SPSS version 22, (Armonk, NY: IBM Corp). Continuous data are presented as means and their associated standard deviation and categorical data are presented as percentages. Group-differences for continuous variables were assessed using the t-test (normal distributed variables), analysis of variance (ANOVA) or Mann-Whitney U test (non-normal distribution). For categorical variables, Chi-square or Fischer’s Exact Tests were used.
We performed our analysis in three steps. First, we used two-way analysis of variance (ANOVA) with implant failure as the dependent variables and the type of implant surface as the independent variable. In the second step, we estimated the mean implant failures after adjusting for relevant co-variables. The relevant co-variables were defined as the ones that showed statistically significant difference between the SLA and RBM Surfaces. As shown in Table 2, these covariates were time of follow-up, diameter and diabetes.
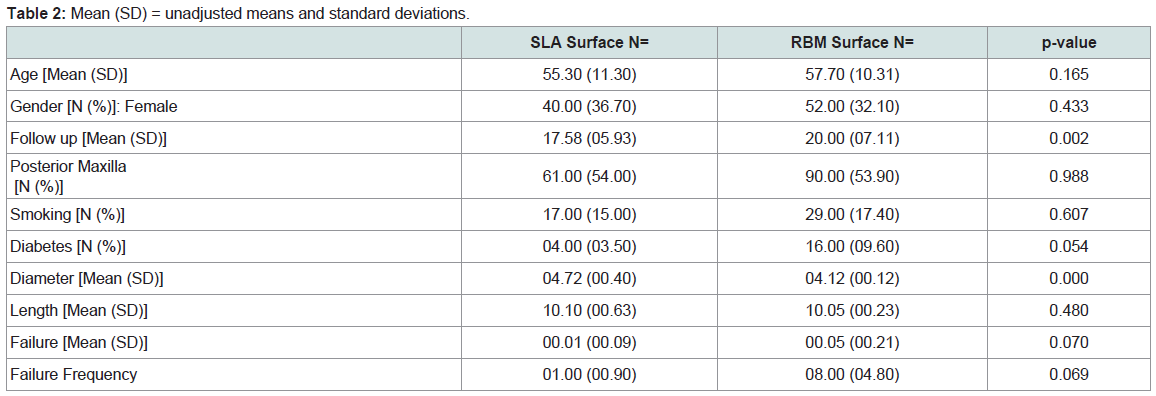
Table 2: Mean (SD) = unadjusted means and standard deviations.
Results
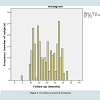
Statistical resultsCharacteristics of the population: Overall, this study evaluated 280 implants that were followed up for a mean of 19.2 month (SD=6.62) and a range of 4-32 months. Figure 3 shows the distribution of the time the implants were followed up. As shown in Table 2, there was a significant difference in the time of follow up between SLA and RBM implants (Table 3). Age, gender, smoking, length of the placed implants, and area of placement (posterior maxilla vs. not-posterior maxilla) did not differ between the two surface groups (Table 2). Diameters of the placed implants were higher in the SLA group and more diabetic subjects were present in the RBM group (Table 4).
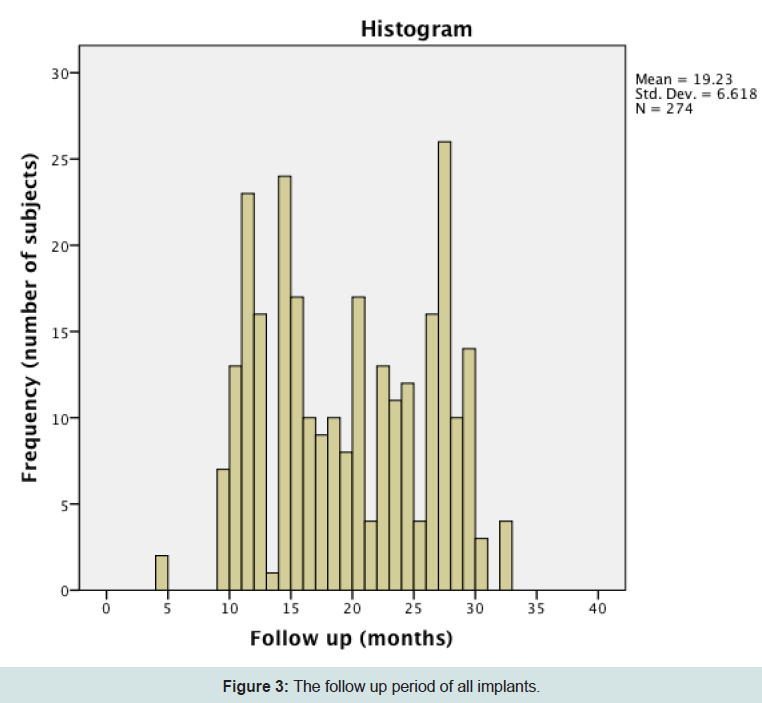
Figure 3: The follow up period of all implants.
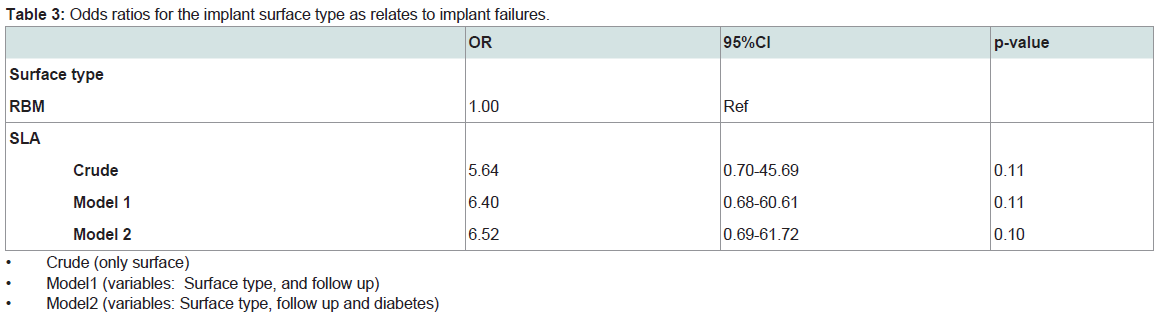
Table 3: Odds ratios for the implant surface type as relates to implant failures.
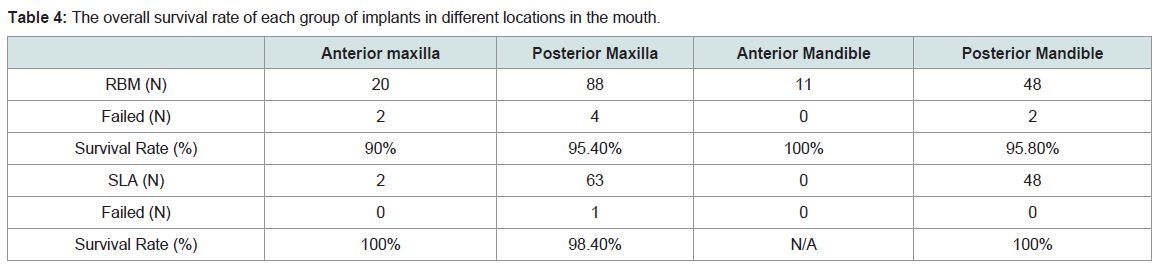
Table 4: The overall survival rate of each group of implants in different locations in the mouth.
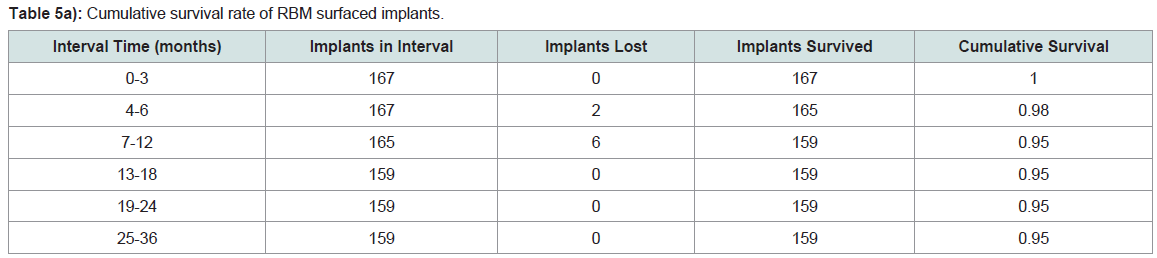
Table 5a: Cumulative survival rate of RBM surfaced implants.
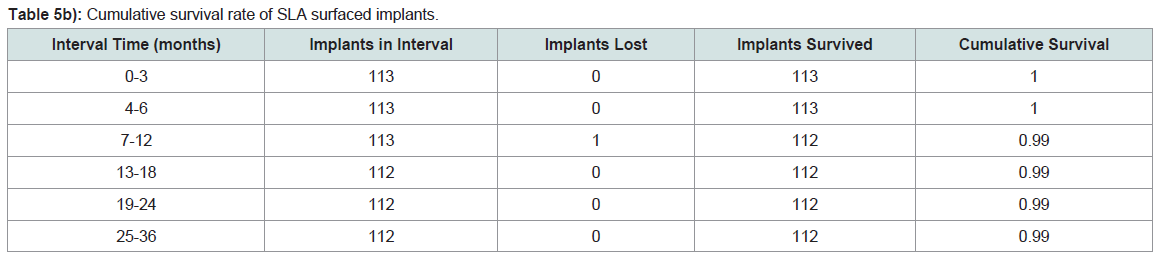
Table 5b: Cumulative survival rate of SLA surfaced implants.
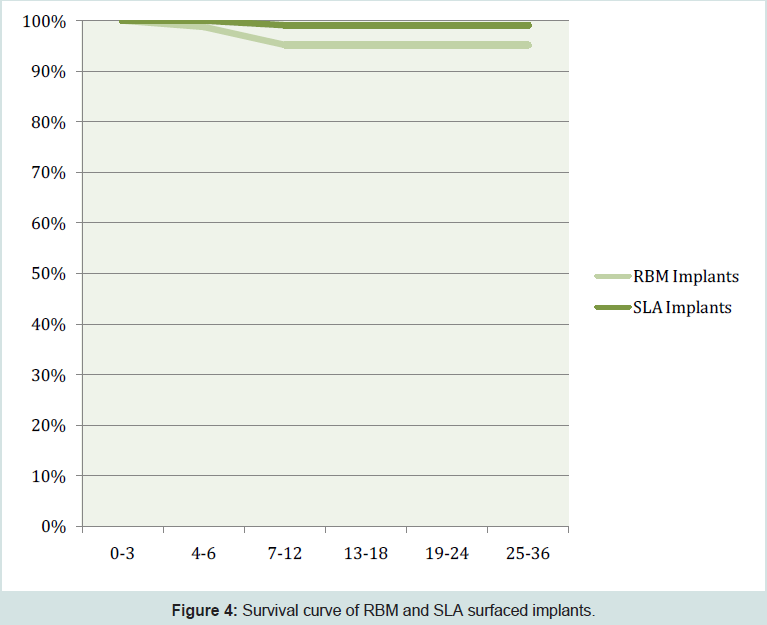
Figure 4: Survival curve of RBM and SLA surfaced implants.
Description of the implant survival by locationAnterior maxilla: Twenty RBM implants were placed in the anterior maxilla. Three of them were placed in grafted sites while the rest were placed in pristine bone. The survival rate for these RBM implants was 90%. Two implants from RBM group that have failed were both of them placed in grafted sites. By comparison two SLA implants placed in the anterior maxilla. One implant was placed in pristine bone while the other was placed in grafted site. The survival rate of these implants was 100%.
Posterior maxilla: Eighty-eight RBM implants were placed in the posterior maxilla. Forty-eight of them were placed in grafted sites utilizing either sinus elevation or guided bone regeneration. The survival rate for these implants was 95.4%. Four implants in this group have failed and all were placed in grafted sites. On the contrary, sixty-three SLA implants were placed in the posterior maxilla. These implants a survival rate of 98%. Twenty-seven of these implants were placed in grafted sites utilizing either guided bone regeneration of sinus augmentation procedure. Only one implant has failed in this group, which was also placed in previously grafted area.
Anterior mandible: In this location eleven RBM surfaced implants were placed. None of these implants were lost during the follow up. No SLA surfaced implants were placed in this location.
Posterior mandible: All of the implants that were placed in the posterior mandible were placed in pristine bone. Forty-eight RBM surfaced implants had a survival rate of 95.8% with two implant failures. Failures, while forty-eight SLA surfaced implants that were placed in the posterior mandible had survival rate of 100%.
Cement-retained verses screw-retained
Screw retained restoration was utilized in the majority of implant restorations. Thirty-nine implants were restored utilizing cement retained restorations and all of which are still in function at the time of this study. All of the failures have occurred in the screw-retained restorations with eight failures in the RBM surface group and one failure in the SLA surface group.
Single unit verses multi units
Out of two hundred and eighty implants placed, seventy-two of them had a single unit restoration. The rest of the implants were supporting fixed dental prosthesis. The survival rate of implants supporting single unit restoration was 100% for the RBM group as well as the SLA group. All of the nine failures have occurred in implants supporting fixed dental prosthesis.
Discussion
The purpose of this study was to evaluate and discuss the difference in survival rates between two geometrically identical implant groups with two different surfaces to help understand the effect of implant surface roughness on implant survival rate. Our results showed that the implant failure was higher in RBM group compared to the SLA group and these results were significant (p=0.039) and could not be explained by the anatomical features of the implant (length, diameter), time of follow up or systemic conditions such as diabetes. Consistent with these findings, the regression analysis showed showed but only at trend level that the RBM implant could be six times more likely to result in failure compared to SLA. An additional significant finding and consistent with the literature was that the longer time the implant is followed up, the least likelihood that the implant would fail. The authors believe that there is a direct relationship between the poor bone quality and the increased rate of failures especially for RBM implants placed in augmented bone. Four out of eighty eight RBM surfaced implants have failed in grafted posterior maxilla. These failed implants were the most distal implants supporting fixed dental prostheses. The remaining forty implants, which were placed in native bone in the posterior maxilla, have all survived. Barone et al. have also reported that implants in grafted posterior maxilla have a higher failure rate compared to implants placed in pristine bone in the posterior maxilla [24]. However, their study did not address the effect of the implant surface on the survival rate.In this study sixty-three SLA implants were placed in the posterior maxilla, only one of them has failed. The failure has occurred in a smoker and the implant was the most distal unit of a maxillary fixed dental prosthesis. The authors suggest that the rougher SLA surface have a compensating effect in areas with poor bone quality through the improved bone-implant-contact which might increase the survival rate at such area compared to less rough RBM surface especially during the first months of osseointegration. This finding has been supported with many previous studies, which investigated the effect of surface roughness on the survival rate of dental implants in poor bone quality. One study compared the survival rate of machined and double acid etched implants. Implants and stated that machined implants had higher failure rate than double acid etched in areas of poor bone quality [22]. Stach et al. have also reported similar results analyzing the survival rate of the same previous two surfaces (Machined vs. double acid etched) [25]. In a recent long term retrospective study of 19 years follow up, it was shown that minimally rough surface implant had higher failure rate than moderately rough surface implants (Machined vs. SLA). The failures were more correlated to implants placed in type IV bone. It was also found that rough surface implants had more failures in the longterm than smooth surfaces, which was correlated to the occurrence of peri-implantitis assessed by probing depth, bleeding on probing, suppuration, Plaque Index, and the presence of saucer- or cratershaped bone loss in radiographs [26].
The survival rate of the RBM implants in the anterior area was 90%, which is low with regard to the short observation period of this study. It has been shown before that the anterior maxilla follows the posterior maxilla in the tendency of implant failures [27]. In addition to that, the two failed implants in the RBM group were placed in previously grafted sites. On the contrary, there were only two SLA implants placed in this area and they were both still in function.
In the posterior mandible, RBM implants had survival rate of 95.8%, as two implants from this group has failed in one patient, while SLA implants had a 100% survival rate. The same survival rate of SLA implants in posterior mandible have been reported previously including short implants [28]. Only two implants from the RBM group have failed. Based on this result, the authors suggest that the degree of implant surface roughness between the two groups does not seem to have an effect on implant survival rate at the posterior mandible at least for the short term outcomes.
Forty-eight RBM surfaced implants and twenty-seven SLA implants were placed in grafted posterior maxilla. Five out of total nine failures have happened in this location. Interestingly, about 50% of the failures occurred in the most distal supporting implant. The number of failure had indirect relationship with the amount of remaining crestal bone before the augmentation. It has been reported in the literature that the most posterior implant receives the highest occlusal forces. The combination of poor bone quality and excess forces on the posterior implant seemed to have a major negative effect on the survival especially for the RBM surface group.
In addition, six out of the nine failures have occurred when the implants were opposing to natural teeth. Parel et al. have also reported an increase in the percentage of implant failure in posterior maxilla with poor bone quality where implants are opposed by natural dentition. They attributed the failures to the irregularities in the occlusion of the natural dentition [29].
This study included twenty-seven smoker subjects. Only three of the implants placed in those subjected had failed and all of the three implants were RBM surfaced implants. Previous studies have reported increased risk of implant failure in smokers [30]. However, in this study the author relates the failure of these implants to local factors like bone quality and occlusal factors rather than the smoking status or any other systemic factors. One possible explanation for this is that the short-term follow up of this study may have prevented the smoking from manifesting a significant effect on the survival rate.
It has been stated before that implant failures occur as a cluster in small number of patients rather than random incidence. This means that some groups of patients have higher risk of losing more implants than others. Multiple factors have been suggested to influence the increased failure rate in these patients. In this study, three RBM implants have failed in one patient. After the removal of these implants, Three SLA implants have been placed. Until the time of this study all of them are still in satisfactory status. Burt et al. have reported that if an implant failure has happened in a patient there is more than 30% chance that this patient will lose another implant [31].
Conclusion
Within the limitation of this study, geometrically identical implants with either RBM or SLA surface have a very comparable survival rates at least in the short term. However, the SLA surface seems to be superior in the posterior maxilla with poor bone. Since the overall failure rate is very low, more studies with higher subjects number and longer follow up are needed.References
- Branemark PI, Breine U, Adell R, et al. (1969) Intraosseous anchorage of dental prostheses. I. Experimental studies. Scand J Plast Reconstr Surg 3: 81-100.
- Mavrogenis AF, Dimitriou R, Parvizi J, Babis GC (2009) Biology of implants osseointegration. J Musculoskelet Neuronal Interact 9: 61-71.
- Iezzi G, Vantaggiato G, Shibli JA, Fiera E, Falco A, et al. (2012) Machined and sandblasted human dental implants retrieved after 5 years: a histologic and histomorphometric analysis of three cases. Quintessence Int 43: 287-292.
- Novaes AB Jr, de Souza SL, de Barros RR, Pereira KK, Iezzi G, et al. (2010) Influence of implant surfaces on osseointegration. Braz Dent J 21: 471- 481.
- Kunzler TP, Huwiler C, Drobek T, Vörös J, Spencer ND (2007) Systematic study of osteoblast response to nanotopography by means of nanoparticle-density gradients. Biomaterials 28: 5000-5006.
- Wennerberg A, Albrektsson T (2009) Effects of titanium surface topography on bone integration: a systematic review. Clin Oral Impl Res 20: 172-184.
- Fan Z, Jia S, Su JS (2010) Influence of surface roughness of titanium implant on core binding factor alpha 1 subunit of osteoblasts. Zhonghua Kou Qiang Yi Xue Za Zhi 45: 466-470.
- Buser D, Schenk R, Steinemann S, Fiorellini J, Fox C, et al. (1991) Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J Biomed Mater Res 25:889-902.
- Wennerberg A, Albrektsson T (2010) On implant surface: A review of current knowledge and opinions. Int J Oral Maxillofac Implants 25: 63-74.
- Block MS, Gardiner D, Kent JN, Misiek DJ, Finger IM, et al. (1996) Hydroxyapatite-coated cylindrical implants in the posterior mandible: 10-year observations. Int J Oral Maxillofac Implants 11: 626-633.
- Watson CJ, Tinsley D, Ogden AR, Russell JL, Mulay S, et al. (1999) A 3 to 4 year study of single tooth hydroxylapatite coated endosseous dental implants. Br Dent J 187: 90-94.
- 12.Esposito M, Hirsch JM, Lekholm U, Thomsen P (1997) Failure patterns of four osseointegrated oral implant systems. J Mater Sci Mater Med 8: 843-847.
- Roccuzzo M, Bonino F, Bonino L, Dalmasso P (2011) Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: Comparative results of a prospective study on two different implant surfaces. J Clin Periodontol 38: 738-745.
- Coelho PG, Granjeiro JM, Romanos GE, Suzuki M, Silva NR, et al. (2009) Basic research methods and current trends of dental implant surfaces. J Biomed Mater Res B Appl Biomater 88: 579-596.
- Buser D, Janner SF, Wittneben JG, Brägger U, Ramseier CA, et al. (2012) 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. Clin Implant Dent Relat Res 14: 839-851.
- Simonis P, Dufour T, Tenenbaum H (2010) Long-term implant survival and success: a 10-16-year follow-up of non-submerged dental implants. Clin Oral Implants Res 21: 772-777.
- Sanz A, Oyarzún A, Farias D, Diaz I (2001) Experimental study of bone response to a new surface treatment of endosseous titanium implants. Implant Dent 10: 126-131.
- Ricci JL, Kummer FJ, Alexander H, Casar RS (1992) Technical note: Embedded particulate contaminants in textured metal implant surfaces J Appl Bio 3: 225-230.
- Novaes AB Jr, Souza SL, de Oliveira PT, Souza AM (2002) Histomorphometric analysis of the bone-implant contact obtained with 4 different implant surface treatments placed side by side in the dog mandible. Int J Oral Maxillofac Implants 17: 377-383.
- Kim YK, Kim BS, Yun PY, Mun SU, Yi YJ, et al. (2014) The seven-year cumulative survival rate of Osstemimplants. J Korean Assoc Oral Maxillofac Surg 40: 68-75.
- Al Nawas B, Hangen U, Duschner H, Krum menauer F, Wagner W (2007) Turned, ma- chined versus double-etched dental implants in vivo. Clinical Implant Dentistry & Related Re- search 9: 71-78.
- Khang W, Feldman S, Hawley CE, Gunsol ley J (2001) A multi-center study comparing dual acid-etched and machined-surfaced implants in various bone qualities. J Periodontol 72: 1384-1390.
- Li D, Ferguson SJ, Beutler T, Cochran DL, Sittig C, et al. (2002) Biomechanical comparison of the sandblasted and acid-etched and the machined and acid-etched titanium surface for dental implants. J Biomed Mater Res 60: 325-332.
- Barone A, Orlando B, Tonelli P, Covani U (2011) Survival rate for implantsplaced in the posteriormaxilla with and without sinusaugmentation: a comparativecohort study. J Periodontol 82: 219-226.
- Stach RM, Kohles SS (2003) A meta-analysis examining the clinical survivability of machined-surfaced and osseotite implants in poor-quality bone. Implant Dent 12: 87-96.
- Han HJ, Kim S, Han DH (2014) Multifactorial evaluation of implant failure: a 19-year retrospective study. Int J Oral Maxillofac Implants 29: 303-310.
- Tolstunov L (2007) Implant zones of the jaws: implant location and related success rate. J Oral Implantol 33: 211-220.
- French D, Larjava H, Ofec R (2014) Retrospective cohort study of 4591 Straumann implants in private practice setting, with up to 10-year follow-up. Part 1: multivariate survival analysis. Clin Oral Implants Res.
- Parel SM, Phillips WR (2011) A risk assessment treatment planning protocol for the four implant immediately loaded maxilla: preliminary findings. J Prosthet Dent 106: 359-366.
- Twito D, Sade P (2014) The effect of cigarette smoking habits on the outcome of dental implant treatment. Peer J 2: e546.
- Weyant R, Burt B (1993) An assessment of survival rates and within-patient clustering of failures for endosseous oral implants. J Dent Res 72: 2-8.