
International Journal of Otorhinolaryngology
Download PDF
Case Report
*Address for Correspondence: Kris R. Jatana, Department of Otolaryngology-Head and Neck Surgery, Nationwide Children's Hospital and Wexner Medical Center at Ohio State University, 555 S. 18th Street, Suite 2A, Columbus, OH 43205-2264, USA, Tel: 614-722-6600; Fax: 614-722-6609; E-mail: Kris.Jatana@nationwidechildrens.org
Citation: Merrill T, Francom C, Kris RJ and Chiang T. Delayed Presentation of Nasal Septal Abscess in a Pediatric Patient Following Infectious Mononucleosis and Acute Bacterial Sinusitis. Inter J Otorhinolaryngology. 2017;4(1): 3.
Copyright © 2017 Merrill T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology| ISSN: 2380-0569 | Volume: 4, Issue: 1
Submission: 2 February, 2017 | Accepted: 8 March, 2017 | Published: 15 March, 2017
 Incision and drainage of the abscess with evacuation of purulent fluid was performed and cultures were obtained. A standard hemitransfixion incision was used. The abscess cavity was full of necrotic debris and the cartilaginous septum was absent. It was thoroughly irrigated until clear. Endoscopic sinus surgery was then performed, addressing the primary site of infection in the sphenoid and ethmoid sinuses. The septal mucosal flaps were approximated and the incision was loosely closed to permit drainage. Cultures grew methicillin susceptible S. aureus, Prevotella, Candida and Fusobacterium. The pediatric infectious disease team assisted with antibiotic management and clinical surveillance. The patient was started on intravenous ampicillin/sulbactam and fluconazole while inpatient and recovered without complication. She was discharged six days postoperatively on oral amoxicillin/clavulanate and fluconazole for four weeks until her Erythrocyte Sedimentation Rate (ESR) andC-Reactive Protein (CRP) normalized and her clinical symptoms resolved. Within two weeks of discharge, her white blood cell count had normalized to 6,600/mL. Despite septoplasty at the time of drainage of the NSA, early follow up demonstrated lack of tip support consistent with saddle nose deformity. Subsequent reconstructive rhinoplasty to correct her saddle nose deformity was completed on postoperative day 67 with a rib autograft.
Incision and drainage of the abscess with evacuation of purulent fluid was performed and cultures were obtained. A standard hemitransfixion incision was used. The abscess cavity was full of necrotic debris and the cartilaginous septum was absent. It was thoroughly irrigated until clear. Endoscopic sinus surgery was then performed, addressing the primary site of infection in the sphenoid and ethmoid sinuses. The septal mucosal flaps were approximated and the incision was loosely closed to permit drainage. Cultures grew methicillin susceptible S. aureus, Prevotella, Candida and Fusobacterium. The pediatric infectious disease team assisted with antibiotic management and clinical surveillance. The patient was started on intravenous ampicillin/sulbactam and fluconazole while inpatient and recovered without complication. She was discharged six days postoperatively on oral amoxicillin/clavulanate and fluconazole for four weeks until her Erythrocyte Sedimentation Rate (ESR) andC-Reactive Protein (CRP) normalized and her clinical symptoms resolved. Within two weeks of discharge, her white blood cell count had normalized to 6,600/mL. Despite septoplasty at the time of drainage of the NSA, early follow up demonstrated lack of tip support consistent with saddle nose deformity. Subsequent reconstructive rhinoplasty to correct her saddle nose deformity was completed on postoperative day 67 with a rib autograft.
Delayed Presentation of Nasal Septal Abscess in a Pediatric Patient Following Infectious Mononucleosis and Acute Bacterial Sinusitis
Tyler Merrill1, Christian Francom2,3, Kris R. Jatana2,3* and Tendy Chiang2,3
- 1The Ohio State University College of Medicine, USA
- 2Department of Pediatric Otolaryngology, Nationwide Children's Hospital, USA
- 3Department of Otolaryngology-Head and Neck Surgery, Wexner Medical Center at Ohio State University, USA
*Address for Correspondence: Kris R. Jatana, Department of Otolaryngology-Head and Neck Surgery, Nationwide Children's Hospital and Wexner Medical Center at Ohio State University, 555 S. 18th Street, Suite 2A, Columbus, OH 43205-2264, USA, Tel: 614-722-6600; Fax: 614-722-6609; E-mail: Kris.Jatana@nationwidechildrens.org
Citation: Merrill T, Francom C, Kris RJ and Chiang T. Delayed Presentation of Nasal Septal Abscess in a Pediatric Patient Following Infectious Mononucleosis and Acute Bacterial Sinusitis. Inter J Otorhinolaryngology. 2017;4(1): 3.
Copyright © 2017 Merrill T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
International Journal of Otorhinolaryngology| ISSN: 2380-0569 | Volume: 4, Issue: 1
Submission: 2 February, 2017 | Accepted: 8 March, 2017 | Published: 15 March, 2017
Abstract
Introduction: The clinical presentation of infectious mononucleosis includes several head and neck manifestations, but does not commonly include sinonasal manifestations. In addition, it is rare for a nasal septal abscess to develop as sequelae of sinusitis. We report a unique case where a pediatric patient developed acute bacterial sinusitis and a nasal septal abscess following an episode of infectious mononucleosis. This is the first reported case of infectious mononucleosis resulting in complicated acute sinusitis with nasal septal abscess.Case presentation: A 16-year-old otherwise healthy Caucasian female presented with infectious mononucleosis and subsequently developed acute bacterial sinusitis. She then developed persistent nasal pain, nasal obstruction, and on exam was found to have bilateral septal fullness with nasal obstruction consistent with a nasal septal abscess. Emergent surgical intervention to drain the abscess followed by systemic antibiotics and delayed reconstructive rhinoplasty.
Conclusion: This case shows that even in the absence of trauma, nasal septal abscess must be considered in patients presenting with persistent nasal pain, obstruction and congestion. This is important for primary care providers, emergency medicine physicians and other health care professionals triaging patients with this constellation of symptoms so that prompt referral may be made to a specialist forappropriate care. This case also suggests that infectious mononucleosis can leave a patient more susceptible to bacterial super infection via inflammatory immune modulation.
Keywords:
Mononucleosis; Abscess; Sinusitis; Pediatric sinusitis; Nasal septal abscessAbbreviations
EBV: Epstein-Barr Virus; NSA: Nasal Septal Abscess; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; MSSA: Methicillin Susceptible Staph AureusIntroduction
Epstein-Barr Virus (EBV) is the primary causative agent of infectious mononucleosis. It is common and widespread in the United States; however, there are few reports of mononucleosis complicated by bacterial sinusitis [1].Nasal Septal Abscess (NSA) was first described in 1810 when Cloquet identified and drained an abscess of the septum and noted a septal perforation [2]. NSA develops when pus collects in the submucoperichondrial plane resulting in ischemia of the underlying cartilaginous septum. Necrosis of the septum often follows which results in nasal septal perforation and or saddle nose deformity and propagation of the infection can lead to serious complications such as cavernous sinus thrombosis, orbital cellulites, or bacteremia [3]. To avoid these complications, standard of care treatment for NSA includes antibiotics and prompt drainage [4]. It is rare to see NSA develop as a result of acute bacterial sinusitis - a literature search revealed only nine such case reports, all of which were in pediatric patients [5-9]. None of these cases document NSA following the diagnosis of infectious mononucleosis. We report a case of NSA following acute bacterial sinusitis as a complication of infectious mononucleosis.
Case Presentation
A 16-year-old Caucasian female presented to the emergency department of a tertiary care children's hospital with a seven-day history of sore throat, fatigue, and difficulty swallowing following three days of treatment with amoxicillin and prednisone. Physical exam revealed tonsillar hypertrophy with oropharyngeal exudates and bilateral cervical lymphadenopathy consistent with infectious mononucleosis; this was confirmed with a positive Monospot test. She was provided supportive care and discharged home. Her amoxicillin was discontinued at this time given the known viral etiology of her symptoms.Six days later, the patient presented to an outside hospital complaining of neck pain, headache, nausea, intermittent vomiting, sore throat, and fatigue. The patient also reported nasal congestion, drainage, facial pain, and a fever. Physical exam was again notable for fever, tonsillar hypertrophy, oropharyngeal exudate and bilateral cervical lymphadenopathy. She did not have purulent nasal drainage or a bulging nasal septum on exam. A Lumbar Puncture (LP) was performed, which was normal. A Computed Tomography exam (CT) of the sinus showed sphenoid and ethmoid sinus opacification but no abscess. Blood work was remarkable for atypical lymphocytes but was otherwise normal. White blood cell count was 4500/mL. After LP and CT, her parents opted to transfer her to a tertiary care children's hospital for further evaluation. Upon arrival, she was nontoxic appearing, and her fever was 37.6 degrees Celsius. Due to her clinical improvement and benign lumbar puncture, it was determined that she could safely be treated on an outpatient basis. She was prescribed a ten-day course of Cefdinir and fluticasone for her sphenoethmoidal sinusitis and discharged home with outpatient follow up in the pediatric otolaryngology clinic.
Within one week the patient called reporting worsening headaches, nasal obstruction, and nasal drainage. She presented acutely to the pediatric otolaryngology clinic for evaluation. Physical exam at this time revealed bilateral nasal obstruction due to septal fullness that was tender and fluctuant on palpation, consistent with a NSA. Given the atypical presentation of infectious mononucleosis, acute bacterial sinusitis and NSA, repeat sinus CT was performed for peri-operative planning to identify the primary source of infection and to rule out intracranial spread. Her white blood cell count was elevated to 14,100/mL. CT demonstrated fluid tracking from the posterior ethmoid air cells and right sphenoid sinus to the nasal septum Figure 1. CT was also noted to show symmetric enhancement of the cavernous sinuses. MRI was then obtained at the recommendation of neurosurgery to further evaluate the potential of intracranial involvement. MRI showed that there was no fluid or empyema in either the epidural or subdural spaces. She was taken to the operating room that day for intervention, which consisted of incision and drainage of the NSA with endoscopic sinus surgery.
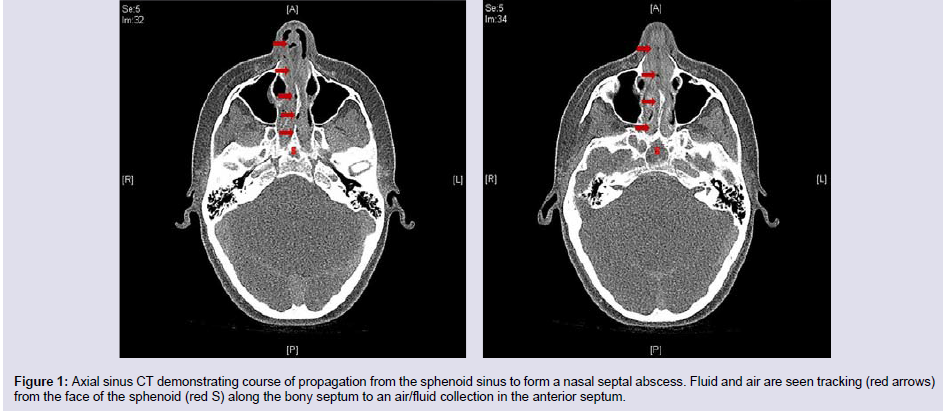
Figure 1: Axial sinus CT demonstrating course of propagation from the sphenoid sinus to form a nasal septal abscess. Fluid and air are seen tracking (red arrows) from the face of the sphenoid (red S) along the bony septum to an air/fluid collection in the anterior septum.
Discussion
Infectious mononucleosis is a common viral illness most commonly associated with lymphadenopathy, pharyngitis, headache, and malaise. It is rarely accompanied by otolaryngologic complications with only 4 patients (0.9%) reported as having sinonasal manifestations [5,10]. However, it should be noted that some authors have suggested infectious mononucleosis can leave a patient more susceptible to bacterial super infection via inflammatory immune modulation [11-13]. No specific pattern of sinus involvement has been reported in EBV mononucleosis complicated by sinusitis.Symptoms of infectious mononucleosis typically resolve in 2-4 weeks, but complete resolution of clinical manifestations can take up to 2 months. Our case demonstrates the importance of close follow up and counseling during this prolonged recovery period, with our patient developing signs of NSA in her third week of illness following initiation of antibiotic therapy. Uncommon manifestations such as nasal pain and obstruction should not be associated with the common clinical signs and would require additional evaluation.
NSA can present either unilaterally or bilaterally. Nasal trauma resulting in hematoma with subsequent infection is the most common etiology for NSA [4]. Some other etiologies include nasal surgery, sinusitis, and dental infection. Physical exam is diagnostic showing a bulging, fluctuant mass in the septum resulting in nasal obstruction and pain. Nasal pain, congestion, headache and fever are common symptoms of NSA.Treatment of NSA typically involves combined medical and surgical management of the necrotic septal tissue with drainage and debridement and reconstruction if needed [13]. Dispenza reports that drainage with immediate reconstruction yields favorable outcomes [14]. Alshaikh and Menger support this conclusion, yet there is no consensus [3,13]. Bilateral nasal packing is suggested to prevent recurrence; a Penrose or rubber band drain may also be useful. Postoperatively, patients are prescribed broad-spectrum antibiotics. Antibiotic therapy is continued for one to two weeks in most cases, but a longer course may be indicated depending upon the severity of the infection and the response to treatment.
The majority of NSA cases are caused by Methicillin Susceptible Staph Aureus (MSSA) [15]. Other bacteria that may be involved are: H. influenzae, Beta-Hemolytic Streptococcus, Streptococcus pneumoniae, and anaerobes [14,15]. Identification of infectious agents should direct antimicrobial treatment.
Conclusion
Though NSA is rare, the severity of complications mandates serious consideration. Failure to quickly diagnose and treat NSA can lead to underdevelopment of the face and restricted nasal airway, as well as other more immediate life-threatening conditions [3,15]. The case presented here suggests that physicians should consider NSA when a patient presents with persistent nasal pain, congestion and obstruction. It is imperative to do an intranasal exam to look for a bulging nasal septum. It is important to remember that a nasal septal abscess may develop in the absence of trauma. The overlap of non-specific symptoms common to NSA, acute bacterial sinusitis, and infectious mononucleosis may cause a delay in diagnosis, but as this case shows, one does not preclude the others. Diagnosis can be made definitively by standard anterior intranasal exam and early intervention is crucial.References
- Shkalim V, Shoval DS, Amir J (2007) Acute sinusitis complicating infectious mononucleosis in an adolescent. Int J Pediatr Otorhinolaryngol Extra 2: 211-214.
- Pirsig W (1984) Historical notes and actual observations on the nasal septal abscess especially in children. Int J Pediatr Otorhinolaryngol 8: 43-54.
- Alshaikh N, Lo S (2011) Nasal septal abscess in children: from diagnosis to management and prevention. Int J Pediatr Otorhinolaryngol 75: 737-744.
- Ambrus PS, Eavey RD, Baker AS, Wilson WR, Kelly JH (1981) Management of nasal septal abscess. Laryngoscope 91: 575-582.
- Zielnik-Jurkiewicz B, Sosinska OO, Fudalej P (2005) Nasal septal abscess and palatine process of the maxilla abscess complicating acute rhinosinusitis in a 12-year old boy. Otolaryngol Pol 59: 865-869.
- Lin IH, Huang IS (2007) Nasal septal abscess complicated with acute sinusitis and facial cellulitis in a child. Auris Nasus Larynx 34: 241-243.
- Hassani R, Aderdour L, Maliki O, Boumed A, Elfakiri MM, et al. (2011) Nasal septal abscess complicating acute sinusitis in a child. Arch Pediatr18: 15-17.
- Huang YC, Hung PL, Lin HC (2012) Nasal septal abscess in an immunocompetent child. Pediatr Neonatol 53: 213-215.
- Beck AL (1945) Abscess of the nasal septum complicating acute ethmoiditis. Arch Otolaryngol 42: 275-279.
- Johnsen T, Katholm M, Stangerup SE (1984) Otolaryngological complications in infectious mononucleosis. J Laryngol Otol 98: 999-1001.
- Neerhout R (1976) Clinical memoranda sinusitis and periorbital infections complicating infectious mononucleosis. Am J Dis Child 130: 777.
- Dearth JC, Rhodes KH (1980) Infectious mononucleosis complicated by severe Mycoplasma pneumoniae infection. Am J Dis Child 134: 744-746.
- Menger DJ, Tabink IC, Trenite GJ (2008) Nasal septal abscess in children: reconstruction with autologous cartilage grafts on polydioxanone plate. Arch Otolaryngol Head Neck Surg 134: 842-847.
- Dispenza C, Saraniti C, Dispenza F, Caramanna C, Salzano FA (2004) Management of nasal septal abscess in childhood: our experience. Int J Pediatr Otorhinolaryngol 68: 1417-1421.
- Canty PA, Berkowitz RG (1996) Hematoma and abscess of the nasal septum in children. Arch Otolaryngol Head Neck Surg 122: 1373-1376.