
Journal of Nutrition & Health
Download PDF
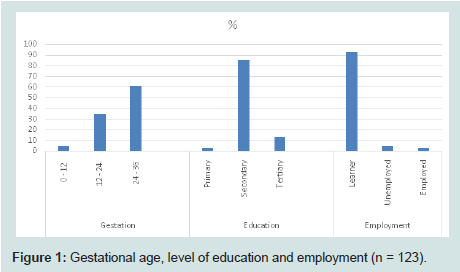 Figure 1: Gestational age, level of education and employment (n = 123).
Figure 1: Gestational age, level of education and employment (n = 123). 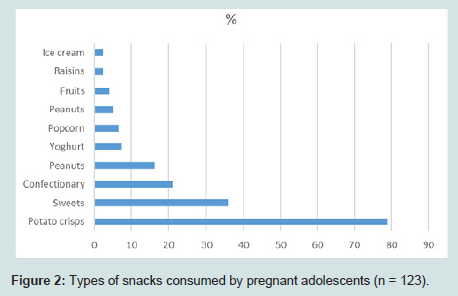 Figure 2: Types of snacks consumed by pregnant adolescents (n = 123).
Figure 2: Types of snacks consumed by pregnant adolescents (n = 123). 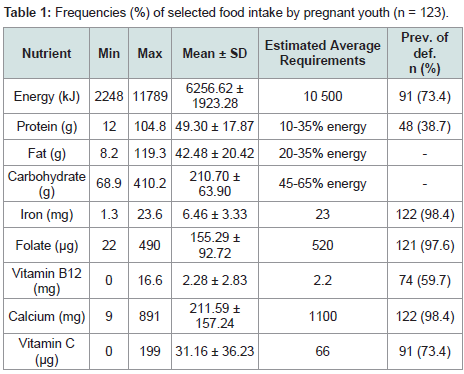 Table 1: Frequencies (%) of selected food intake by pregnant youth (n = 123).
Table 1: Frequencies (%) of selected food intake by pregnant youth (n = 123). 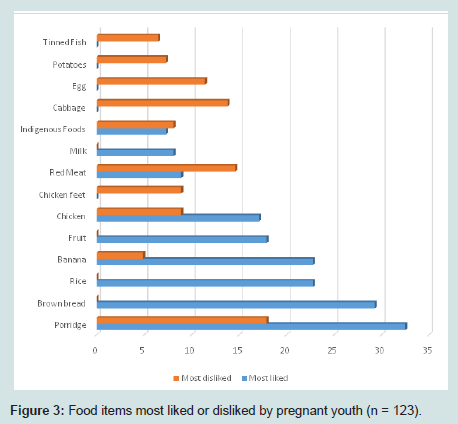 Figure 3: Food items most liked or disliked by pregnant
Figure 3: Food items most liked or disliked by pregnant 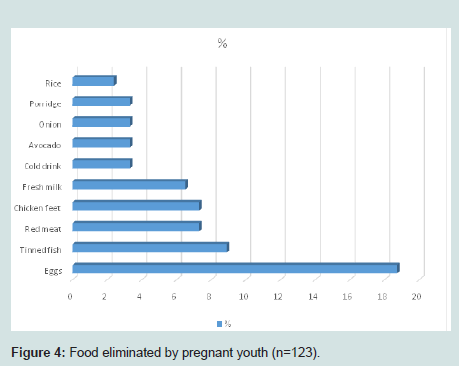 Figure 4: Food eliminated by pregnant youth (n=123).
Figure 4: Food eliminated by pregnant youth (n=123). 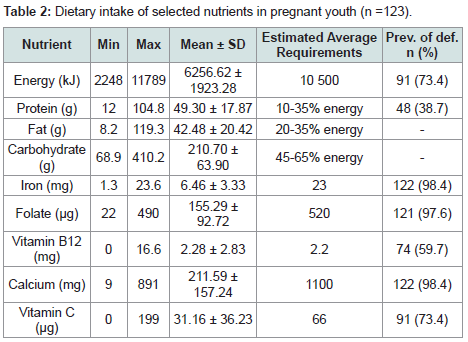 Table 2: Dietary intake of selected nutrients in pregnant youth (n =123).
Table 2: Dietary intake of selected nutrients in pregnant youth (n =123).
Research Article
Dietary Patterns and Food Behaviours of Pregnant Youth: A Survey in the Polokwane Local Municipality of Limpopo Province, South Africa
Bopape MM1, Alberts M2 and Mbhenyane XG3*
- 1Department of Human Nutrition, University of Limpopo, South Africa
- 2Department of Medical Sciences, University of Limpopo, South Africa
- 3Division of Human Nutrition, University of Stellenbosch, South Africa
**Address for Correspondence: Mbhenyane XG, Division Human Nutrition, Faculty of Medicine and Health Sciences, University of Stellenbosch, Tygerberg, South Africa, Tel: +27219389135; Fax: +27219389868; E-mail: xgm@sun.ac.za
Citation: Bopape MM, Alberts M, Mbhenyane XG. Dietary Patterns and Food Behaviours of Pregnant Youth: A Survey in the Polokwane LocalMunicipality of Limpopo Province, South Africa. J Nutri Health. 2018;4(1): 6.
Copyright © 2018 Bopape MM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Nutrition and Health | ISSN: 2469-4185 | Volume: 4, Issue: 1
Submission: 16 May 2018 | Accepted: 25 June 2018 | Published: 28 June 2018
Abstract
Youth pregnancy continues to be a public health concern in South Africa, while nutrition during the first thousand days has become a focus of child and maternal focus and interventions. The study aimed to determine the food behaviours and dietary patterns of pregnant youth in the Polokwane Local Municipality of Limpopo province. It was a descriptive, exploratory and quantitative study. The study was conducted at five randomly selected primary health care clinics in the Polokwane Local Municipality, Limpopo province and pregnant youth aged between fifteen and twenty one years were recruited from these clinics. Sociodemographic data were collected using a validated questionnaire and dietary data were collected using a repeated twenty four hour recall and selected food frequency questionnaire. Blood was also collected to determine serum levels for iron, folate and vitamin B12. The food frequency questionnaire only included foods that are high in iron, folate and vitamin B12 as well as those food items that can enhance or inhibit iron absorption. Pregnant youth had an average of two meals per day, with breakfast being the most commonly skipped meal. There was generally less snacking as compared to studies conducted in urban areas. The nutrient intake was less than 67% of the estimated average requirements for energy, iron, folate, calcium and vitamin C and Vitamin B12. The diet was predominantly cereal-based, with a very low intake of fruit, vegetables and animal products.
Keywords
Food behaviours; Dietary patterns; Pregnant teenagers
Introduction
Pregnancy during adolescence, intended or unintended, remains a global public health concern according to the World Health Organization and is associated with low socioeconomic status and with increased risk both to mother and foetus [1]. Foetal complications that occurs more commonly in teenage pregnancies include low birth weight, infection, growth restriction and sudden infant death syndrome [2].
According to McCarthy et al. complications during pregnancy and childbirth are the second highest cause of death in 15-19-yearold females globally [3]. The adaptive changes that occur during foetal organ development in response to malnutrition may permanently alter adult physiology and metabolism, which is beneficial to survival under conditions of limited nutrient intake, but detrimental when nutrients are abundant [3,4]. Late entry by pregnant adolescents into prenatal care, and other sociodemographic, lifestyle and physiological factors have been associated with restricted foetal growth and low birth weight [5].
Teenage pregnancy remains high in many countries, including South Africa. According to Jonas et al. teenage pregnancy in South Africa is a complex problem with a myriad of contributing factors including poverty, gender, inequalities, poor access to health services and facilities and inadequate health education [6]. Khuzwayo and Taylor have reported that the South African government, civil society and non-governmental associations have developed several interventions in response to the complexity of the problem and to attempt to influence the risky behaviours of the youth [7]. Teen pregnancy is known to lead to negative health and social outcomes for both teen mother and child [8].
Pregnant adolescents are particularly vulnerable to under nutrition due to the fact that they are still growing and might not be able to meet both the maternal and foetal needs [9,10]. This is worsened by the fact that adolescents have unique eating patterns that predispose them to inadequate dietary intakes. Studies have shown serious dietary deficiencies with regard to a number of nutrients amongst both pregnant and non-pregnant youth, especially iron, calcium and folate - nutrients that are crucial during pregnancy [11-14]. Whitworth and Cockrill further reported that infant mortality rate, prematurity episodes and gastroenteritis are more likely to occur in children born to adolescent mothers from low socioeconomic groups [15].
Moreover, teen years are associated with erratic eating habits and food behaviours that may result in poor nutrition. Under nutrition during pregnancy is associated with higher mortality and morbidity amongst women and young children. It has also been shown to have a crucial impact on foetal growth [3]. Furthermore, it is now evident that babies who are small or disproportionate at birth, be it due to poor maternal nutritional status or otherwise, have increased rates of coronary heart disease, hypertension, non-insulin dependent diabetes mellitus, insulin resistance syndrome and obesity and are prone to certain cancers later in life [16]. This study therefore assessed the food behaviours and dietary patterns of pregnant adolescents from low socioeconomic environments with an aim to give a deeper understanding of the actual food behaviours in rural environments that may lead to poor pregnancy outcomes.
Materials and Methods
Study design
The study was a descriptive, exploratory and quantitative survey conducted in primary health care clinics in the Mankweng area and surroundings in the Polokwane local Municipality in Limpopo province of South Africa. The study population targeted pregnant teenagers living in Polokwane local municipality in Limpopo province. Mankweng area and surroundings, with a population of 70 022 was used as a sampling frame [17]. There was an estimated 27.6% youth of the total population of Polokwane City at the time with a 52:48 % female to male ratio [17]. Purposive sampling was used and youth attending the four randomly clinics on study days were approached and recruited for the study. Only those pregnant adolescents who gave consent were included in the study, while those who did not return for the completion of the second 24-hr recall were excluded from the final analysis. The final sample group consisted of 130 pregnant youth attending the selected primary health care clinics in Polokwane Local Municipality, Limpopo province. Of the 130 pregnant youth who were recruited and interviewed, only 123 complete data sets were analysed, seven youth did not return for the second interview.
Data collection procedures
A researcher administered questionnaire was used to collect data. The instrument was developed and pilot tested prior to data collection. The measurements collected included: general information on sociodemographic data, dietary patterns assessed using a 24-hour recall, general food behavior questions and a food frequency checklist. The 24-hour recall was carried out twice, one on a weekday and the other on a Sunday in order to obtain a good estimate of dietary intakes. The food frequency questionnaire was used to determine frequency of consumption of food high in iron, folate and vitamin B12. Inadequate intake of these nutrients is associated with the development of anaemia. A general section was included in the questionnaire to determine food likes and dislikes and those foods that participants eliminated during pregnancy.
The questionnaire was administered by a trained dietitian, who was one of the researchers, and blood samples were collected by a professional nurse. The data were collected over seven months in an attempt to recruit more subjects. The youth were shown food models in order to make it easier for them to estimate the amounts of food consumed. In cases where food models could not be used, household measurements such as teaspoons and tablespoons were used and these were converted into grams by using the conversion figures in the Food Quantity Manual [17]. Blood samples were also collected by a trained Nursing professional for analysis of iron, folate and vitamin B12 status.
Ethical considerations
Ethical approval was granted by the ethics committee of the University of Limpopo and permission to use the primary health care clinics was granted by the research committee of the Limpopo Department of Health and Social Development in South Africa. Clinic management was also requested to give permission and allocate a consultation room in which the study could be conducted. The aims and procedures of the study were explained and those who were willing to participate signed the consent forms. The parents of adolescents under the age of 18 years were requested to provide permission prior to data collection. The adolescent were free to withdraw at any time during the study. The study followed the ethical principles as outline in the Helsinki Declaration and the Constitution of South Africa.
Data analysis
Dietary intakes were summarised using minimum and maximum values, means and standard deviations. Intakes were compared with the Estimated Average Requirements (EAR) for pregnancy and levels of intake lower than 67% of the EAR were considered deficient [13]. All the data on the general questionnaire and those pertaining to eating habits were coded and summarised as frequency counts and percentages. Each item on the food frequency questionnaire was coded and the responses were expressed as daily, weekly, or monthly and never consumed. Items that were consumed weekly were further divided into the following categories: once to twice per week; thrice to four times per week and five to six times per week. Lists of foods liked and disliked by youth as well as those eliminated during pregnancy were compiled. The number of meals and snacks were summarized using means and standard deviations. Snacks were considered as those meals consumed between the three main meals. The Food Finder program was used to analyse nutrient intakes. Statistical analysis was done using SPSS 18.0. Iron, folate and vitamin B12 status has been reported in another article [18,19].
Results
Demographic data and participants characteristics
The youth were from four villages situated 30 km east of Polokwane city and a radius of 10 km from the University of Limpopo in the rural areas of the province with inadequate infrastructure such as roads and running water, but the houses were electrified. They all lived with their parents at the time of the study. Subjects were dividedinto two age categories, namely 12-18 years (38%) and 19-21 years (62%), to accommodate the differences in nutrient needs for the iron, folate and vitamin B12 analysis. The majority (61%) of the youth were in the third trimester of their pregnancies, while 34% and 5% were in the second and first trimesters respectively. Most (84.6%) were learners attending secondary or high school, 13% were at tertiary institutions and 2.4% had left school. Only 2.4% were employed; 4.9% were unemployed and 92.7% was still at school (Figure 1).
Food behaviours and dietary patterns
Youth ate an average of two meals per day (2.6 meals per day) and very few had snacks on a daily basis (0.4 times per day). The types of snacks most liked by the subjects were potato crisps, sweets, confectionery (baked goods), peanuts and yoghurt. Few youth chose healthier snacks such as fruit (4%) and raisins (2.4%) (Figure 2).
Results from the food frequency questionnaire showed that the food items consumed by most youth on a daily basis was tea, followed by oranges, raw tomato, egg, milk, coffee and orange juice. About 48% of youth reported that they never eat liver, 26.8% did not eat red meat and 19.5% ate neither spinach nor indigenous vegetables. Green leafy vegetables were consumed on a daily basis by only 2.4% of the youth. Raw cabbage was also not commonly consumed, as indicated by the fact that 55.3% of the subjects reported never eating it raw; 15.4% ate it once a week (Table 1). When asked to list the items most liked, porridge, brown bread and rice were the top three items mentioned. Approximately 17.9% of the youth reported that they liked fruit and bananas, in particular were found to be more popular than other fruit. Foods of animal origin were low on the list. Vegetables were also not commonly eaten. The subjects were also asked to list the food items they disliked most (Figure 3). Of the food items disliked by these youth, the majority were from the meat group, with red meat being at the top of the list, followed by egg, chicken feet and tinned fish. Other food groups, in descending order, were vegetables, cereal and fruit. Very few subjects mentioned the fats and oils group, sugar, milk and legume groups. The pregnant youth eliminated eggs, tinned fish, red meat and chicken feet since having fallen pregnant (Figure 4). Some of the reasons given for eliminating food items included nausea and vomiting caused by food items such as fried food and onions, taboos against the use of milk, liver, eggs and food aversions, especially to red meat, eggs, tinned fish and chicken feet.
The mean energy and protein intake for the whole group of subjects was 60% and 82% of the EAR respectively. Fat contributed 27%, carbohydrates 59% and protein 14% of the total energy intake. There was inadequate intake of most micronutrients, with the mean calcium, iron, folate and vitamin C intakes below EAR (Table 2). Data on the percentage of youth who had inadequate dietary intake are also presented in (Table 2).
Discussion
Youth ate an average of two meals per day, fewer than the traditional three meals per day. The most commonly skipped meal was breakfast, a pattern also observed in other studies [9,20]. Snacking was not as common as found by Steyn, et al. who observed a higher degree of snacking in youth from urban areas and less snacking among youth from rural areas in South Africa [21]. The lower number of meals and lack of snacks between meals could have led to the low energy intake amongst the subjects in the present study. Whisner, et al. conducted a survey on 66 pregnant adolescents in the United States of America (USA) and reported commonly liked foods to be fast foods, candy, fried chicken and pizza, similar in composition to those reported in this study, i.e. potato crisps, sweets, confectionary, peanuts and yoghurt [20]. Others also reported a diet comprising of high-sugar snacks, fast foods and convenience foods in pregnant youth in the USA [5].
The energy intake of the subjects was low (< 67% of the EAR), with 14%, 27% and 59% of energy as protein, fat and carbohydrates respectively. Most of the energy came from carbohydrates, with fat contributing less than 30% of energy. Similarly, low intake of energy by pregnant youth was reported in the USA but with a different distribution of 13%, 34% and 53% from protein, fats and carbohydrates respectively [22]. The higher fat proportion in the latter study was related to a higher meat intake, which was very low in the present study. A combination of the low fat-intake and a predominantly cereal-based diet could have led to the low energy-intake amongst the subjects in the present study. Their low energy-intake predisposes these youth to poor weight gain and thus puts them at risk of having low birth weight or preterm babies.
Protein intake exceeded 67% of the EAR and most of the sources were plant-based, as reported in another study conducted in a low socioeconomic area [23]. Plant-based proteins are known for their low biological value and if not taken with starches, which are able to complement their limited amino acid content, a deficiency of essential amino acids could result [24]. Essential amino acids are necessary for growth and development of the foetus as demonstrated in a study that evaluated the amino acid levels in adolescent pregnancies and showed that lower levels were associated with adverse perinatal outcomes [24]. Again, meat is known as the best source of amino acids and failure to include it in the diet could lead to inadequate dietary intake if proper substitution is not done.
Almost all (98.4%) of the subjects had inadequate iron intake. When asked which food items they have eliminated since having fallen pregnant, red meat, tinned fish and eggs, which are good sources of iron and protein, were amongst the top five mentioned. Those who liked meat rarely ate it because of its cost. Very few youth ate meat more than three times per week and the portion sizes were mostly restricted to as low as 30g, especially in the case of red meat. Most of these subjects reported that they ate meat only once per week, the most popular being chicken. Liver, which is also a good source of iron and folate, was very unpopular amongst the subjects, with 48% reporting that they never eat it. Low socioeconomic status may have contributed to the low meat intake. On the other hand, pregnant women are known to dislike meat [25]. Whisner, et al. reported that the majority (56.1%) of the pregnant teens in their study did not make any dietary changes and that those who did eliminated chicken [20]. In contrast, Wise reported that pregnant teens drank more water, ate a large variety of foods and limited soft drinks due to pregnancy [9]. In the Wise study pregnant teens avoided fruit and vegetables they had liked before due to heartburn and morning sickness and they also stopped eating protein foods such as tuna and chicken. Our findings on chicken avoidance by pregnant teens therefore concur with those of Whisner, et al. and Wise [9,20].
The folate intake by subjects was low despite the consumption of spinach and indigenous vegetables by some, which are known to be rich in folate. The consumed portion sizes of these folate-rich foods were small and they were only eaten on average twice per week. Only 2.4% of the youth reported eating these vegetables every day and 19.5% of the youth never ate them. Xie, et al. have also reported low levels of fruit and vegetable intake among pregnant youth in the USA [26].
Only one subject had adequate calcium intake. Very few (7.3%) consumed milk, the cheapest source of calcium, every day and 20% of the subjects never consumed it. The reasons given for no consumption of include “milk consumption during pregnancy being a taboo”, while others stopped taking milk to avoid diarrhea. Poor calcium intakes were also reported amongst pregnant Iranian women and Zuni Indian adolescents [16,27].
The low vitamin C intake among subjects is a reflection of the poor intake of fruit and vegetables, common amongst youth. In the current study the most consumed fruits were bananas, which are not rich sources of vitamin C. In studies where vitamin C intake was reported to be higher, it was mainly from fortified flavoured drinks and not from fruit and vegetables [27,28]. The vitamin C content of drinks consumed by subjects in this study was not analysed.
In summary, youth had an average of two meals per day and breakfast was the most commonly skipped meal. There was also generally less snacking as compared to studies conducted in more developed or urban areas [29,30]. The nutrient intake in this study was less than 67% of the EAR for energy, iron, folate, calcium and vitamin C, in contrast with findings of low intake of vitamin D, vitamin E, magnesium and calcium by Lee, et al. [5]. Youth had a predominantly cereal-based diet, with a very low intake of fruit, vegetables and animal products, including milk. The prevalence of anaemia in this study was high (36%), with iron deficiency anaemia being the most prevalent (57%) as compared to either folate (9%) or vitamin B12 (7%) deficiency anaemia as previously reported by these researchers [19]. There was a significant difference (p = 0.03) in serum folate between teenagers who were receiving folic acid supplements and those who were not receiving any such supplements [19].
Some of the limitations were that this study did not establish compliance to folate and iron supplements issued at the clinics; it was assumed that the youth consumed them. The youth were recruited from the clinics where it is standard operating procedure to issue iron and folate supplements to pregnant women. Furthermore, birth outcomes were not determined as this was across-sectional study. The low sample size might be a limiting factor, but many studies have used similarly low numbers of subjects (100 pregnant teens by Ngaha, et al. in Cameroon [12]; 66pregnant teens by Whisner, et al. in the USA, 14 pregnant teens by Wise in the USA [9,20]; 156 pregnant teens by Lee, et al. in the USA [5]; and 39 pregnant teens by Guzel, et al. in Turkey [24]. Only longitudinal studies focusing on pregnancy outcomes have reported sample sizes larger than 500. It is possible that the low samples sizes are a reflection of the fact that teens are already stressed by pregnancy and are unlikely to participate in research that is perceived as invading their privacy. Furthermore, this study did not explore factors that influence food behaviours, but other studies have reported food choices to be influenced by hunger, cravings, food availability and money [5]. Davis, et al. have indicated that behaviours of food consumption are similar between mothers and toddlers and caution that unhealthy eating patterns are likely to be passed to children, potentially putting them at additional risk of negative health consequences [31].
Dietary intake was inadequate and lacking in most of the key nutrients crucial during pregnancy and this poor intake may have detrimental effects on pregnancy. A high prevalence of anaemia was reported. Health professionals need to start paying more attention to pregnant youth in as far as sound nutrition habits are concerned. These youth need to be educated about the South African food-based dietary guidelines and the dangers of skipping meals, especially breakfast, as nutrient intake during the rest of the day may not compensate for skipping this meal. It is recommended that Dieticians/Nutritionists should give talks at primary health care clinics and schools, to ensure that most youth, both pregnant and non-pregnant, get the appropriate nutritional message. Future studies should follow up the pregnant youth from conception until postpartum to determine the impact of dietary practices including factors influencing food behaviours on birth outcomes.
References
- Mccarthy PF, O’brienU, Kenny L (2014) The management of teenage pregnancy. BMJ 349: g5887.
- Balayla J, Azoulay L, Assayag J, Benjamin A, Abenhaim HA (2011) Effect of maternal age on the risk of stillbirth: A population-based cohort study on 37 million births in the United States. Am J Perinatol 28: 643-650.
- Erkkola M, Karppinen M, Järvinen A, Knip M, Virtanen SM (1998) Folate, vitamin D, and iron intakes are low among pregnant Finnish women. Eur J Clin Nutr 52: 742-748.
- Barker DJ, Martyn CN, Osmond C, Hales CN, Fall CH (1993) Growth in utero and serum cholesterol concentrations in adult life. BMJ 307: 1524-1527.
- Lee S, Young BE, Cooper EM, Pressman E, Queenan RA, et al. (2014) Nutrient inadequacy is prevalent in pregnant adolescents, and prenatal supplement use may not fully compensate for dietary deficiencies. ICAN: Infant, Child, & Adolescent Nutrition 6: 152-159.
- Jonas K, Crutzen R, van der Borne B, Sewpal R, Reddy P (2016) Teenage pregnancy rates and associations with other health risk behaviours: a three-wave cross-sectional study among South African school-going adolescents. Reprod Health 13: 50.
- Khuzwayo N, Taylor M (2018) Exploring the socio-ecological levels for prevention of sexual behaviours of the youth in uMgungundlovu district municipality, Kwazulu-Natal. Afr J Prim Health Care Fam Med 10: 1-8.
- Rosenberg M, Pettifor A, Miller WC, Thirumurthy H, Emch M, et al. (2015) Relationship between school dropout and teen pregnancy among rural South African young women. Int J Epidemiol 44: 928-936.
- Wise NJ (2015) Pregnant adolescents, beliefs about healthy eating, factors that influence food choices, and nutrition education preferences. J Midwifery Womens Health 60: 410-418.
- Scholl TO, Hediger Ml, Schall JI, Khoo CS, Fischer Rl (1994) Maternal growth during pregnancy and the competition for nutrients. Am J Clin Nutr 60: 183-188.
- Case AP, Adrienne T, Canfield MA, Wilkinson AV (2015) Periconceptional risk factors for birth defects among younger and older teen mothers. J Pediatr Adolesc Gynecol 28: 263-270.
- Ngaha DW, Fombang EN, Ejoh RA (2014) Dietary intake of vitamin A and macronutrients among pregnant women in Ngaoundere Town, Adamawa Region, Cameroon. Food Nutr Sci 5: 2071-2080.
- Beard JL (1994) Iron deficiency: Assessment during pregnancy and its importance in pregnant adolescents. Am J Clin Nutri 59: 502S-510S.
- Steyn NP, Wicht Cl, Rossouw JE, van wyk Kotze, TJ, van Eck M (1989) Nutritional status of 11-year old children in the Western Cape. I. Dietary intake. South African J Food Sci Nutr 1: 15-20.
- Whitworth M, Cockerill R (2010) Antenatal management of teenage pregnancy. Obstetrics Gynaecology Reproductive Medicine 20: 323-328.
- Houshiar-Rad A, Omidvar N, Mahmoodi M, Kolahdooz F, Amini M (1998) Dietary intake, anthropometry and birth outcome of rural pregnant women in two Iranian districts. Nutr Res 18: 1469-1482.
- Statistics South Africa (2012) Census 2011 Census in brief. Pretoria.
- Food Finder 3 (2002) Dietary analysis software program, version 1.0.7. Cape Town; South African Medical Research Council.
- Bopape MM, Mbhenyane XG, Alberts M (2008) The prevalence of anaemia and selected micronutrient status in pregnant youth of Polokwane Municipality in the Limpopo Province. South Afr J Clin Nutr 21: 332-336.
- Whisner CM, Bruening M, O’brien KO (2016) A brief survey of dietary beliefs and behaviours of pregnant adolescents. J Pediatr Adolesc Gynecol 29: 476-481.
- Steyn NP, Wicht Cl, Rossouw JE, van wyk Kotze TJ, Laubscher R (1990) The eating pattern of adolescents in the Western Cape. South Afr J Food Sci Nutr 2: 23-27.
- Dwyer JT, Evans M, Stone EJ, Feldman HA, Lytle L, et al. (2001) Adolescents’ eating patterns influence their nutrient intakes. J Am Diet Assoc 101: 798-802.
- Patel RC, Lamparelli RD, Sacks AJ, Breeds AD, Macphail AP, et al. (1992) Nutritional anaemia in pregnant black women in Soweto. South Afr J Food Sci Nutr 4: 29-32.
- Guzel AI, Cinar M, Erkilinc S, Aksoy RT, Yumusuk OH, et al. (2015) Association between adverse perinatal outcomes and amino acid levels measured with nutrient questionnaire in adolescent pregnancies. J Chin Med Assoc 79: 335-339.
- Rao KM, Balakrishna N, Laxmaiah A, Venkaiah K, Brahmam GN (2006) Diet and nutritional status of adolescent tribal population in nine states of India. Asia Pac J Clin Nutr 15: 64-71.
- Xie Y, Madkour AS, Harville EW (2015) Preconception nutrition, physical activity, and birth outcomes in adolescent girls. J Pediatr Adolesc Gynecol 28: 471-476.
- Cole SM, Teufel-Shone NI, Ritenbaugh CK, Yzenbaard RA, Cockerham Dl (2001) Dietary intake and food patterns of Zuni adolescents. J Am Diet Assoc 101: 802-806.
- Giddens JB, Krug SK, Tsang RC, Guo S, Miodovnik M, et al. (2000) Pregnant adolescent and adult women have similarly low intakes of selected nutrients. J Am Diet Assoc 100: 1334-1340.
- Liu Y, Zhai F, Popkin BM (2006) Trends in eating behaviours among Chinese children (1991-1997). Asia Pac J Clin Nutr1 5: 72-80.
- Steyn NP, Badenhorst CJ, Nel JH (1993) The meal pattern and snacking habits of schoolchildren in two rural areas of Lebowa. South Afr J Food Sci Nutr 5: 5-9.
- Davis AM, Gallagher K, Taylor M, Canter K, Gillette MD, et al. (2013) An in-home intervention to improve nutrition, physical activity and knowledge among low-income teen mothers and their children: Results from a pilot study. J Dev Behav Pediatr 34: 609-615.