
Journal of Integrative Medicine & Therapy
The Influence of Functional Electrical Stimulation during Cycling Exercise on Cardiorespiratoric Response in Order of Cadence at Increasing and Persistent Exercise in Healthy Adults
Lutz Baumgärtel1*, Nico Nitzsche2 and Henry Schulz3
- 1Lutz Baumgärtel, M.Sc, Institute of Human Movement Science and Health, Chemnitz University of Technology, Thüringer Weg 11: 021A, 09126, Chemnitz, Germany, Tel: +49 371 531-34365; Fax: +49 371531-834365; E-mail: Lutz.baumgaertel@hsw.tu-chemnitz.de
*Address for Correspondence: Lutz Baumgärtel, M.Sc, Institute of Human Movement Science and Health, Chemnitz University of Technology, Thüringer Weg 11: 021A, 09126, Chemnitz, Germany, Tel: +49 371 531-34365; Fax: +49 371 531-834365; E-mail: Lutz.baumgaertel@hsw.tu-chemnitz.de
Citation: Citation: Baumgärtel L, Nitzsche N, Schulz H. The Influence of Functional Electrical Stimulation during Cycling Exercise on Cardiorespiratoric Response in Order of Cadence at Increasing and Persistent Exercise in Healthy Adults. J Integrative Med Ther. 2016;3(1): 4.
Copyright © 2016 Baumgärtel L, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Integrative Medicine & Therapy | Volume: 3, Issue: 1 |
Submission: 25 March 2016 | Accepted: 13 April 2016 | Published: 18 April 2016
Reviewed & Approved by: Dr. Harold H. Fain, University of North Texas Health Science Center, USA
Abstract
Introduction: Functional electrical stimulation during cycling (FES Cycling) exercise is seen to improve cardiorespiratoric performance for maintaining health in patients with spinal cord injury. The relationship between widely varying stimulation pattern, functional movement and effects on cardiorespiratory response is not yet sufficiently studied. While different muscle activation patterns during the FES Cycling may increase metabolic consumption, the influence of different cycling cadences is controversial. The aim of this study was to investigate the acute effect of functional electrical stimulation and different cadences on cardiorespiratoric responses in passive cycling movement in healthy volunteers.
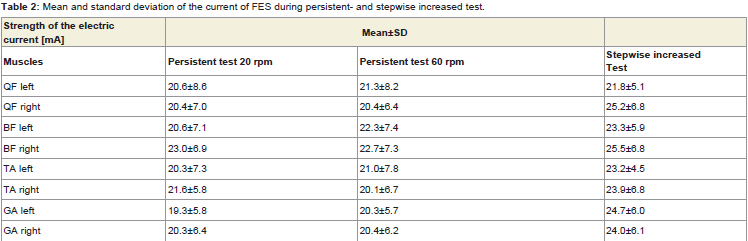
Methodology: 26 healthy subjects assigned in two groups, performed stepwise increased tests with and without functional electrical stimulation with cycling cadence increased from 20-60 rpm, 10 rpm every five minutes and two 25 minutes lasting, persistent tests with functional electrical simulation at cadences of 20 and 60 rpm. Passive cycling exercise was performed adding functional electrical stimulation on musculus quadriceps femoris, biceps femoris, tibialis anterior and gastrocnemius. Subjects were obliged to perform no voluntary movement. Heart rate, oxygen uptake and respiratory exchange ratio was recorded.
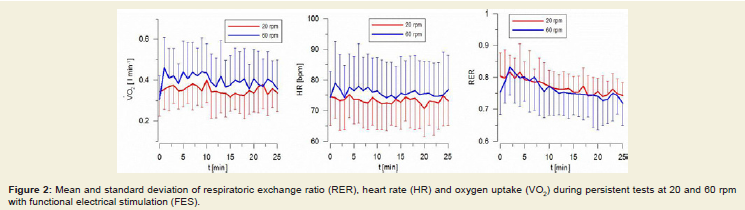
Results: No significant changes between heart rate and oxygen uptake at different cadences during stepwise increased tests were found (p>0.05). Respiratory exchange ratio was different between beginning and end of the test (p<0.05). There was no Influence of electrical stimulation in any of measured parameters (p>0.05). Mean oxygen uptake within persistent 60 rpm test increased significantly, compared to 20 rpm. No differences heart rate and respiratory exchange ratio were detected (p>0.05).
Discussion: Acute cardiorespiratoric responses during passive cycling caused by functional electrical stimulation are only tendential, but not significant. By increasing the current and the cadence of FES Cycling metabolic consumption could be increased. A significant increase in cardiorespiratoric consumption is apparently only possible by combining exercises using FES Cycling and active arm exercise.
Keywords
Functional electrical stimulation; FES Cycling; Cardiorespiratory fitness; Cycling cadence
Introduction
Functional electrical stimulation is been used for about 50 years in treatment and rehabilitation of patients with stroke and spinal cord injury. Numerous studies could show positive effects of functional electrical stimulation (FES) combined with cycling movement (FES Cycling) [1,2]. Main improvements in stroke patients are motor changes, such as improving walking ability, balance and spasticity [3-5]. Increase of residual muscle strength, prevention of contractures and sense of well-being are described as important therapeutic goals in paraplegia [6,7]. Improvement of cardiorespiratory performance seems to be a considerable component for maintaining health [8], especially in patients with spinal cord injury. FES Cycling exercises interventions show significant improvements in cardiorespiratory parameters [9,10]. Investigations with simple electromyostimulation(EMS) without functional movement on cardiac patients with very low cardiac levels also show an increase in cardiorespiratory capacity [2,11]. The relationship between stimulation parameters, functional movement and effects on cardiorespiratory parameters is not yet sufficiently studied.In numerous investigations exercise protocols, stimulation frequencies and strength of electric current varies widely. It is known that rectangular pulses for FES are suitable [12,13]. Basically in both, healthy and paralyzed muscles with increased amperage, more motor units are recruited [14]. While different muscle activation patterns during FES Cycling may increase the cardiorespiratory load, the influence of different cycling cadences is discussed controversial [15,16]. The aim of this study was to investigate the acute effect of functional electrical stimulation and different cadences on cardiorespiratoric responses in passive cycling movement in healthy volunteers.
Methodology
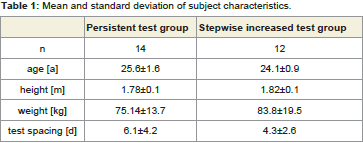
26 healthy volunteers (25±1.5 years, 180±10 cm, 78.8±16.5 kg) were divided into two groups (stepwise increased test group=ST/persistent test group=PT) (Table 1).
Results
Stepwise increased tests (ST)
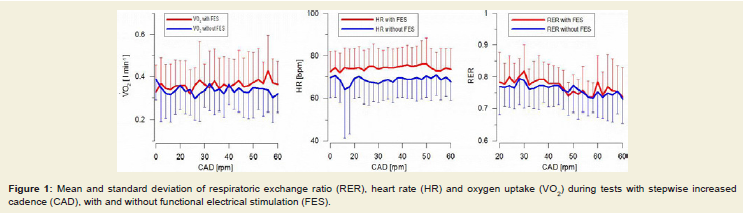
Rest value before the test with FES was recorded 73.1±9.9 beats per minute (bpm) (HR), 0.328±0.129 l min-1 (VO2) and 0.78±0.09 (RER). Before the test without FES the value showed a 2.5±0.20 bpm lower heart rate and a 0.03±0.02 lower RER. Oxygen uptake showed about 0.061±0.029 l min-1 higher values.
Mean value of heart rate, VO2 and RER during measurement with FES was 75.03±9.49 bpm, 0.362±0.131 l min-1 and 0.77±0.07. Without FES the values decreased about 4.95±0.76 bpm, 0.029±0.020 l min-1 and 0.02±0.00. The minimal differences seen in the graphs of HR and VO2 between varying cycling cadences showed no statistical significance (p>0.05) (Figure 1). Only the RER was significantly different between the beginning and end of the stepwise increased tests (p<0.05). No influence of electrical stimulation could be detected in any of the three parameters (p>0.05).
Discussion
FES currently appears to be an important potential therapy in neurological disorders. Therefore neuromuscular electrical stimulation is coupled with a functional movement like cycling or running. Recent findings show effects of interventions with FES Cycling [17]. Adjustments of the neuromuscular system are affected by the specific stimulation of the muscle fibers. Furthermore, changes in the muscle cells are stimulated by influence of the cell metabolism, whereby the utilization of oxygen and the ATP consumption plays an important role.References
- Davis GM, Hamzaid NA, Fornusek C (2008) Cardiorespiratory, metabolic, and biomechanical responses during functional electrical stimulation leg exercise: health and fitness benefits. Artif Organs 32: 625-629.
- van Buuren F, Mellwig KP, Fründ A, Bogunovic N, Oldenburg O, et al. (2014) Elektromyostimulation: verbesserung von lebensqualität, sauerstoffaufnahme und linksventrikulärer funktion bei chronischer herzinsuffizienz. Rehabilitation 53: 321-326.
- Ambrosini E, Ferrante S, Pedrocchi A, Ferrigno G, Molteni F (2011) Cycling induced by electrical stimulation improves motor recovery in postacute hemiparetic patients: a randomized controlled trial. Stroke 42: 1068-1073.
- Lo HC, Tsai KH, Su FC, Chang GL, Yeh CY (2009) Effects of a functional electrical stimulation-assisted leg-cycling wheelchair on reducing spasticity of patients after stroke. J Rehabil Med 41: 242-246.
- Lo HC, Hsu YC, Hsueh YH, Yeh CY (2012) Cycling exercise with functional electrical stimulation improves postural control in stroke patients. Gait Posture 35: 506-510.
- Frotzler A, Coupaud S, Perret C, Kakebeeke TH, Hunt KJ, et al. (2008) High-volume FES-cycling partially reverses bone loss in people with chronic spinal cord injury. Bone 43: 169-176.
- Wilder RP, Jones EV, Wind TC, Edlich RF (2002) Functional electrical stimulation cycle ergometer exercise for spinal cord injured patients. J Long Term Eff Med Implants 12: 161-174.
- Baumann F, Bloch W, Jäger E (2012) Sport und körperliche Aktivität in der Onkologie. Springer, Berlin Heidelberg.
- Berry HR, Perret C, Saunders BA, Kakebeeke TH, Donaldson Nde N, et al. (2008) Cardiorespiratory and power adaptations to stimulated cycle training in paraplegia. Med Sci Sports Exerc 40: 1573-1580.
- Muraki S, Fornusek C, Raymond J, Davis GM (2007) Muscle oxygenation during prolonged electrical stimulation-evoked cycling in paraplegics. Appl Physiol Nutr Metab 32: 463-472.
- Fritzsche D, Fruend A, Schenk S, Mellwig KP, Kleinöder H, et al. (2010) Elektromyostimulation (EMS) bei kardiologischen Patienten. Wird das EMS-Training bedeutsam für die Sekundärprävention? Herz 35: 34-40.
- Szecsi J, Fornusek C, Krause P, Straube A (2007) Low-frequency rectangular pulse is superior to middle frequency alternating current stimulation in cycling of people with spinal cord injury. Arch Phys Med Rehabil 88: 338-345.
- Szecsi J, Fornusek C (2014) Comparison of torque and discomfort produced by sinusoidal and rectangular alternating current electrical stimulation in the quadriceps muscle at variable burst duty cycles. Am J Phys Med Rehabil 93: 146-159.
- Bickel CS, Gregory CM, Dean JC (2011) Motor unit recruitment during neuromuscular electrical stimulation: a critical appraisal. Eur J Appl Physiol 111: 2399-2407.
- Fornusek C, Davis GM (2008) Cardiovascular and metabolic responses during functional electric stimulation cycling at different cadences. Arch Phys Med Rehabil 89: 719-725.
- Hunt KJ, Ferrario C, Grant S, Stone B, McLean AN, et al. (2006) Comparison of stimulation patterns for FES-cycling using measures of oxygen cost and stimulation cost. Med Eng Phys 28: 710-718.
- Hamzaid NA, Davis GM (2009) Health and fitness benefits of functional electrical stimulation-evoked leg exercise for spinal cord-injured individuals: a position review. Top Spinal Cord Inj Rehabil 14: 88-121.
- Hasnan N, Ektas N, Tanhoffer AI, Tanhoffer R, Fornusek C, et al. (2013) Exercise responses during functional electrical stimulation cycling in individuals with spinal cord injury. Med Sci Sports Exerc 45: 1131-1138.
- Gregory CM, Bickel CS (2005) Recruitment patterns in human skeletal muscle during electrical stimulation. Phys Ther 85: 358-364.
- Ferguson RA, Ball D, Krustrup P, Aagaard P, Kjaer M, et al. (2001) Muscle oxygen uptake and energy turnover during dynamic exercise at different contraction frequencies in humans. J Physiol 536(Pt 1): 261-271.
- Wahl P, Schaerk J, Achtzehn S, Kleinöder H, Bloch W, et al. (2012) Physiological responses and perceived exertion during cycling with superimposed electromyostimulation. J Strength Cond Res 26: 2383-2388.
- Griffin L, Decker MJ, Hwang JY, Wang B, Kitchen K, et al. (2009) Functional electrical stimulation cycling improves body composition, metabolic and neural factors in persons with spinal cord injury. J Electromyogr Kinesiol 19: 614-622.
- Perret C, Berry H, Hunt KJ, Donaldson N, Kakebeeke TH (2010) Feasibility of functional electrical stimulated cycling in subjects with spinal cord injury: an energetic assessment. J Rehabil Med 42: 873-875.