
Journal of Andrology & Gynaecology
Download PDF
Case Report
*Address for Correspondence: Murat Bozkurt, MD, Caucasus University Campus Health Care Research and Development Hospital, KARS, Turkey, Tel: +905322279072/+905056330044; Fax: 0474 225 14 30; E mail: jindrmb@yahoo.com
Citation: Salman S, Bozkurt M, Yumru AE, Bozyigit A, Kavsi B, et al. Laparoscopic Management of Leiomyoma Developing from Rudimentary Horn in Mayer- Rokitansky-Küster-Hauser Syndrome. J Androl Gynaecol. 2013;1(2): 2.
Copyright © 2014 Salman S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Andrology & Gynaecology | ISSN 2332-3442 | Volume: 2, Issue: 1
Submission: 21 October 2013 | Accepted: 19 December 2013 | Published: 27 December 2013
Keywords: Leiomyoma; Congenital uterine anomalies; Mayer- Rokitansky-Küster-Hauser Syndrome; Amenorrhea; Infertility


Laparoscopic Management of Leiomyoma Developing from Rudimentary Horn in Mayer- Rokitansky-Küster-Hauser Syndrome
Suleyman Salman2, Murat Bozkurt1*, Ayse Ender 2,Abdulhamit Bozyigit2,Berker Kavsi2 and Abdulhamit Bozyigit3
- 1Kafkas University Medical Faculty, Department of Obstetrics and Gynecology, Kars, Turkey
- 2Taksim Education and Research Hospital, Department of Obstetrics and Gynecology Istanbul, Turkey
- 3Maternity and Children’ s Hospital, Department of Obstetrics and Gynecology, Sakarya, Turkey
*Address for Correspondence: Murat Bozkurt, MD, Caucasus University Campus Health Care Research and Development Hospital, KARS, Turkey, Tel: +905322279072/+905056330044; Fax: 0474 225 14 30; E mail: jindrmb@yahoo.com
Citation: Salman S, Bozkurt M, Yumru AE, Bozyigit A, Kavsi B, et al. Laparoscopic Management of Leiomyoma Developing from Rudimentary Horn in Mayer- Rokitansky-Küster-Hauser Syndrome. J Androl Gynaecol. 2013;1(2): 2.
Copyright © 2014 Salman S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Andrology & Gynaecology | ISSN 2332-3442 | Volume: 2, Issue: 1
Submission: 21 October 2013 | Accepted: 19 December 2013 | Published: 27 December 2013
Abstract
Various congenital anomalies of the mullerian system have so far, been described. Our case with MRKH syndrome had two rudimentary horns, and had also a leiomyoma arising from the left rudimentary horn. The patient was presented to our department because of primary amenorrhoea and infertility. Clinical examination revealed a blind vaginal pouch of 3 cm in size and mass was palpated in the left adnexal region measuring about 5 cm in size. At the diagnostic laparoscopy examination, two rudimentary horns were observed to be connected to each other with a fibrous band, and there was a leiomyoma measuring 60 × 50 mm in size originating from the left horn, both of the fallopian tubes and ovaries were normal. The leiomyoma was laparoscopically removed. Using this method have led to successful Clinical outcomes. We sought to present the case of the myoma and its laparoscopic management associated with rarely encountered MRKH syndrome. Although rarely encountered, it should be kept in mind that patients with MRKH syndrome may develop leiomyomas from rudimentary horn. And also laparoscopy is recommended for the diagnosis and treatment of this diseases.Keywords: Leiomyoma; Congenital uterine anomalies; Mayer- Rokitansky-Küster-Hauser Syndrome; Amenorrhea; Infertility
Introduction
The prevalence of congenital uterine anomalies appears to be 6.7% in fertile population and it is found 7.3% in an infertile population while it is observed to be 16.7% in those with recurrent miscarriage [1]. Mayer-Rokitansky- Kuster-Hauser (MRKH) syndrome, the most severe anomaly of Mullerian system, was first described by Mayer, Rokitansky, Kuster and Hauser [2]. The etiologic factors of this syndrome is not fully understood, and environmental and genetic factors are thought to play a role [3]. In MRKH syndrome, the vagina and uterus is congenitally absent, both ovaries are of normal size and fallopian tubes are normal, rudimentary uterine horns may be present in this syndrome [4,5]. A case of myoma associated with MRKH syndrome was first reported in 1977 [6]. We sought to present the case of the myoma associated with rarely encountered MRKH syndrome.Case Report
A 41-years old patient presented to Gynecology Department of Taksim Education and Research Hospital because of primary amenorrhea and infertility in 2013. The patient had a past history of primary amenorrhea and some 20 years back she applied to Gynaecology Department but could not know what diagnosis it was. Clinical examination revealed a blind vaginal pouch of 3 cm in size and mass was palpated in the left adnexal region measuring about 5 cm in size. Physical examination revealed normal bilateral breasts, normal axillary and pubic hair patterns. Transabdominal ultrasonography showed a solid mass in the left adnexal region. Chromosomal investigation of our case indicated a normal karyotype of 46, XX. Diagnostic laparoscopy revealed that the uterus was absent and there were two rudimentary horns connected with each other by a fibrous band, and there was myoma-like mass 60 x 50 mm arising from the left rudimentary uterine, both ovaries and fallopian tubes were normal in appearance (Figure 1 and Figure 2). The mass was laparoscopically excised. The patient was discharged the following day, histopathological examination confirmed that the mass was a leiomyoma.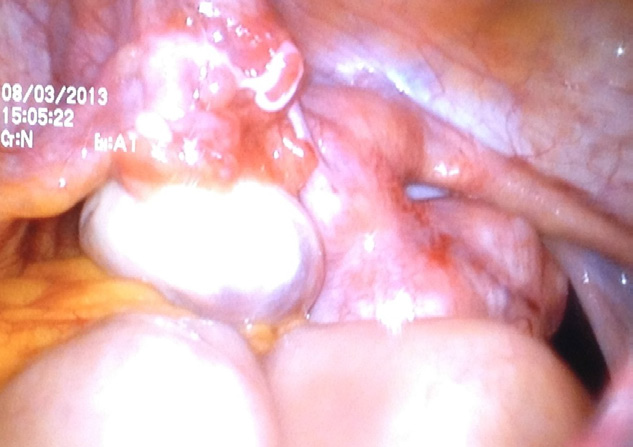
Figure 1: A rudimentary left uterine horn with tube and ovary. A leiomyoma 60 x 50 mm is shown.
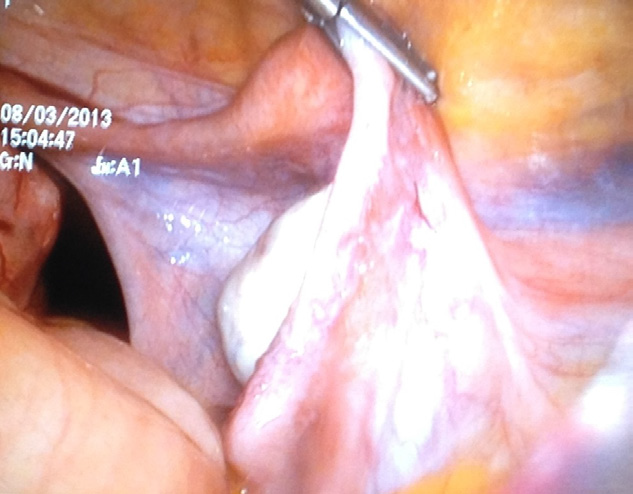
Figure 2: A rudimentary right uterine horn with tube and ovary.
Discussion
Mayer-Rokitansky-Kuster-Hauser (MRKH ) syndrome is a rare disorder described as aplasia or hypoplasia of uterus and vagina due to early arrest in development of Mullerian duct. The incidence reported is one out of 4.500 women[7]. Diagnosis of MRKH syndrome is often delated untill late puberty. The symptoms for presentation are amenorrhea, infertility and pelvic pain. This rare syndrome described as aplasia or hypoplasia of uterus and vagina due to the early arrest in development of Mullerian duct. These patients have the ovaries and fallopian tubes of normal functions and most of whom have also two uterine remnants of different sizes [3]. Incidence of leiomyoma of uterus is very high in the general female population. But only few cases of leiomyoma have been reported in women with MRKH syndrome[8-10].The clinical symptoms associated with the pelvic in patients with MRKH have to be carefully investigated; uterine remnants in patients with MRKH syndrome are composed of fibromuscular tissue and a leiomyoma may develop from this tissue; the cases of uterine leiomyoma developing from uterine remnant have been reported in the literatüre [11]. Leiomyomas of the uterus are estrogen dependent tumours. The etiopathogenesis of leiomyoma from the normal uterus smooth muscle cells is not known. Their growth has been associated with genetic predisposition, hormones and few growth factors. Mullerian ducts have smooth muscle cells at their proximal ends, which probably may lead to the growth of leiomyoma from the rudimentary uterus in MRKH syndrome. However, the exact etiopathogenesis of leiomyoma from the rudimentary uterus in MRKH syndrome is not known [12].
Differential diagnosis of leiomyoma of rudimentary uterus in MRKH syndrome includes ovarian fibroma, gastrointestinal stromal tumour (GIST) of intestine and extravesical leiomyoma of urinary bladder [12].
Myomas originating from uterine remnanats may cause pelvic pain; however, they may not give any indications as it was in our cases and may be detected by diagnostic procedures. Initial investigation in woman with MRKH syndrome with leiomyoma is radiologic modalities like ultrasonography, computed tomography and magnetic resonance imaging. However, laparoscopic evaluation is more accurate to evaluate the pelvic pathologies. Also, laparoscopy can be used as a method of diagnosis and treatment when a pelvic mass is detected in patients with MRKH syndrome. The surgical treatment of leiomyoma can be done by laparoscopy or laparotomy. In the literature, Tsin et al. have first reported the successful laparoscopic management of the 8.5 cm size leiomyoma uterine with MRKH syndrome. Laparoscopy have several advantages compared to laparotomy [13]. The major advantages of laparoscopic surgery are that it provides adequate visualization of the entire abdominal cavity and localization of pathology. And also this methods reduced morbidity, smaller, cosmetically acceptable wounds leads to early recovery. In our case, laparoscopic surgery was done sucessfully and best clinical outcomes were obtained.
In conclusion, leiomyoma may, albeit rarely, develop from uterine remnant, so it must be borne in mind that leiomyoma may be included in the differential diagnosis of patients with MRKH presenting with a pelvic mass. And also we suggested that laparoscopy can be used for the diagnosis and treatment of this disease.
References
- Saravelos SH, Cocksedge KA, Li TC (2008) Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: a critical appraisal. Hum Reprod Update 14: 415- 429.
- Rokitansky K (1838) Uber die sogenannten Verdoppelun- gen des Uterus. Med JB Ost Staates 26: 39- 42.
- Deligeoroglou E, Kontoravdis A, Makrakis E, Christopoulos P, Kountouris A, et al. (2004) Development of leiomyomas on the uterine remnants of twowomen with Mayer- Rokitansky- Kuster- Hauser syndrome. Fertil Steril 81: 1385- 1387.
- Giatras K, Licciardi F, Grifo JA (1998) Laparoscopy for pelvic pain in the Mayer- Rokitansky- Kuster- Hauser syndrome. A case report. J Reprod Med 43: 203-205.
- Cakmak H, Arici A (2006) Mullerian Duct Anomalies. Turkiye Klinikleri J Pediatr Sci 2: 23-29.
- Beecham CT, Skiendzielewski J (1977) Myoma in association with Mayer-Rokitansky- Kuster- Hauser syndrome. Am J Obstet Gynecol129: 346- 348.
- Alfonsa Pizzo, Antonio Simone Laganà, Emanuele Sturlese, Giovanni Retto, et al. (2013) Mayer-Rokitansky-Kuster-Hauser Syndrome: Embryology,Genetics and Clinical and Surgical Treatment. ISRN Obstet Gynecol 2013: 628717.
- Deligeoroglou E, Kontoravdis A, Makrakis E, Christopoulos P, Kountouris A, et al. (2004) Develpoment of leiomymas on the uterine remnants of two women with Mayer-Rokitansky-Kuster-Hauser syndrome. Fertil Steril 81:1385–1387.
- Dandu S, Jones SE, Okeahialam MG (2000) Mayer-Rokitansky-Kuster-Hauser syndrome associated with chromosomal abnormality and fibroidarising from the rudimentary uterine horn. J Obstet Gynecol 20: 98.
- Edmonds DK (2003) Multiple fibroids in a postmenopausal women with Mayer-Rokitansky-Kuster-Hauser syndrome. J Pediatr Adolesc Gynecol 16: 65–66.
- Jadoul P, Pirard C, squifflet J, Smets M, Donnez J (2004) Pelvic mass in women with Mayer- Rokitansky- Kuster- Hauser syndrome. Fertil Steril 81: 203-204.
- Rawat KS, Buxi T, Yadav A, Ghuman SS, Dhawan S (2013) Large leiomyoma in a woman with Mayer-Rokitansky-Kuster-Hauser syndrome. J Radiol CaseRep 7: 39-46.
- Tsin DA, Waters TK, Granato RC (2000) Laparoscopic myomectomy in a patient with Mayer-Rokitansky-Kuster-Hauser syndrome. J Am Assoc Gynecol Laparosc 7: 411-413.